By Raad Shakir, MD

Raad Shakir, MD
If someone anywhere in the world had a stroke or a TIA in the last 60 years, the World Health Organization (WHO) coding system placed the event under either vascular diseases or episodic symptoms, not in the appropriate central nervous system chapter of ICD-10. This situation started with ICD-7 in 1955 and has continued since. It skews all statistics of neurological diseases produced by the WHO. ICD-10 has been in use since 1990, and a total revamp is long overdue. The information is not only stale and old, but incorrect. Codes such as “slow virus infection” for prion diseases are expected to be used in the 21st century?
The WHO Department of Mental Health and Substance Abuse, where neurology sits, commissioned a Neurosciences Topic Advisory Group (Neurology TAG) in 2009. I have had the privilege of chairing the TAG, which expanded to involve specialists from all neuroscience specialties. The tasks were huge and detailed. The aim was to produce ICD-11, which will both serve the needs of the non-specialists as well as those working in highly developed institutions.
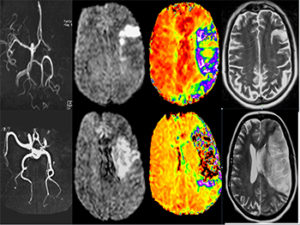
Brain imaging studies capture the evolution of acute ischemic stroke in two patients.
Perhaps the most important ICD-10 anomaly the TAG faced was the situation of cerebrovascular diseases (CVDs) and their future placement in ICD-11. Attempting change of the basic architecture of ICD-10 required a major case to be made on the reasoning and practicality of changing an existing status. CVDs fell under Circulation Disorders on the premise that they are a disease of vessels. Statisticians, following the principle of ascribing disorders to their basic etiology, followed this procedure, ignoring the fact that all of the effects of CVDs are neurological and that the initial interaction of the neurovascular bundle is fundamental to the pathophysiology. Moreover, in ICD-10, other ischemic disorders affecting the eyes, bowels, and kidneys fall under the affected organs. Transient ischemic attacks were classified under episodic disorders separate from CVDs.
This situation is not only incorrect, but it has led to massive confusion of reporting the fact that a leading cause of death is not placed as a disease of the brain. The first act the TAG performed was to contact and agree with our cardiology colleagues as cardiac events were lumped with CVDs, skewing their statistics as much as ours. They were asked to approve a total separation of cardiac and brain diseases for the benefit of both. This was successfully established with the Cardiology TAG in 2011. It, of course, remains that cardiogenic causes of CVDs are appropriately reported in both sections.
Where to Place CVDs?
The WHO statisticians were informed, and we had “initial acquiescence” until the middle of 2016, when a major statistician’s review of ICD-11 was carried out by the WHO Department of Informatics and Statistics. At that time, statistics advisers had second thoughts, which again placed all CVDs under the circulation section of the Joint Linearization for Mortality and Morbidity section of ICD-11.
This decision needed to be reversed, which required intensive lobbying to make the point that stroke is a brain disease. It has to be emphasized that the ICD is “owned” by the WHO statisticians, and our role as clinicians is advisory.
Be that as it may, the TAG had to pursue this matter vigorously and provide the scientific reasoning for the change. WFN and the World Stroke Organization (WSO) acted in a closely coordinated manner. Professor Bo Norrving, past president of the WSO, and I, the representatives of the Neurology TAG, used all possible avenues to make the case for the WHO Department of Informatics and Statistics. In addition to the production of scientific evidence on the etiology of stroke and the interactions between vessels and brain parenchyma, we needed to mobilize other players to reinforce the message of the importance of stroke being classified as a brain disease for resource allocation and training of staff—medical, nursing, and others—to combat the scourge of CVDs.
The issue is vital for the future of neurology, and The Lancet published two letters, one from us1, and the second a reply from the WHO Department of Informatics and Statistics2. We had put forward the argument for stroke moving to the central nervous system, while the ICD classification team put forth its reasoning, quoting continuity and the fact that CVDs were placed in ICD-7 in 1955.
This meant going to governments, as they are the ultimate power in the WHO structure. We are most grateful for the support, such as a most powerful letter from Veronica Skvortsova, the minister of Health of the Russian Federation, addressed to the WHO director general. Dr. Skvortsova is herself a neurologist and therefore is fully aware of this anomaly in ICD-10. We also are most indebted to the health ministries of Austria and New Zealand for their support.
We were hugely supported by patient organizations that wrote to the WHO and to neurologists from across the world for their support. Following all of this effort, a request came from the ICD classification team asking us to have another face-to-face meeting. This was conducted Dec. 21, 2016, in Geneva. The daylong meeting was most interesting as it started with the assertion of the statisticians on the importance of continuity and stability of statistics over decades. This is something crucial to us all. However, explanations were provided with regard to the need for radical change and why it is crucial to rectify a previous anomaly. The WHO technical department where neurology sits was represented by Dr. Tarun Dua, who made the case for the need to place CVDs under the nervous system diseases chapter of the ICD-11. The Neurology TAG was represented by Dr. Norrving and me. The meeting ended without an immediate outcome. We did not know the meeting’s conclusions for more than three months. The WHO ICD team had to clear its decisions with its statistics consultants from around the world. This is perfectly understandable as many computer systems have to be retuned, and this will need time and finance.
Two further medical statistics meetings took place. Finally, on March 31, I was informed by email: “The grouping ‘Cerebrovascular Diseases’ has moved into ‘Diseases of the Nervous System.’” This is a culmination of eight years of work and is the most logical outcome for our endeavors.
Now the world of neurology is correctly represented. This is immediately reflected in the soon-to-be-published “Global Burden of Disease” paper, where in 2015 “neurological disorders rank as the leading cause group of DALYs (disability-adjusted life years) and the second-leading cause of death in the world.” This means that resources will be appropriately allocated not only for CVDs but all neurological disorders. The WHO decision was truly momentous, and for that we are grateful. Stroke is back where it belongs.
References:
- Shakir R, Davis S, Norrving B, Grisold W, Carroll WM, Feigin V, Hachinski V. Revising the ICD: stroke is a brain disease. Lancet 2016; 388:2475-6.
- Boerma T, Harrison J, Jakob R, Mathers C, Schmider A, Weber S. Revising the ICD: explaining the WHO approach. Lancet 2016; 388: 2476-7.



 This year’s World Brain Day commemorates the foundation of the WFN. The prior World Brain Day topics were aimed at epilepsy and dementia, and now it is aimed at stroke. We are partnering this time with the World Stroke Organization (WSO), which puts great global effort into the prevention and treatment of stroke.
This year’s World Brain Day commemorates the foundation of the WFN. The prior World Brain Day topics were aimed at epilepsy and dementia, and now it is aimed at stroke. We are partnering this time with the World Stroke Organization (WSO), which puts great global effort into the prevention and treatment of stroke.