By Chandrashekhar Meshram

Chandrashekhar Meshram
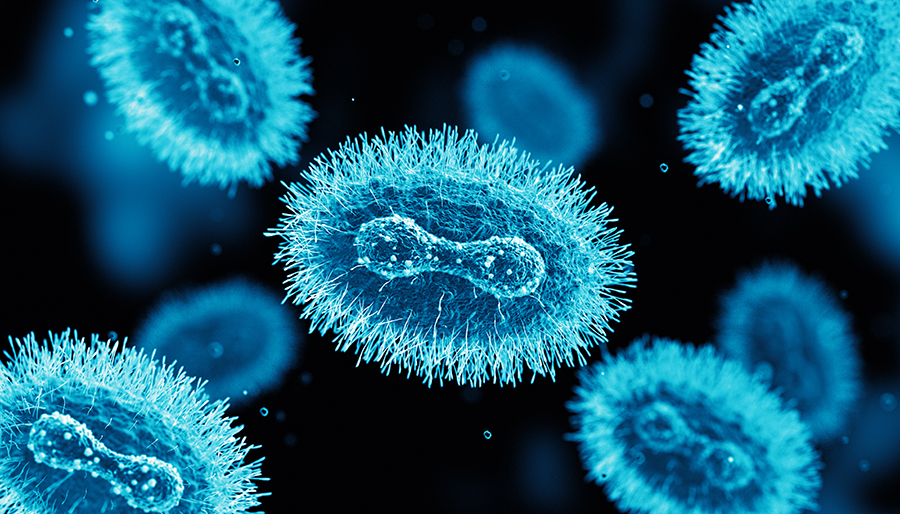
The World Health Organization recently declared monkeypox a global public health emergency of international concern. Monkeypox is a viral zoonosis caused by a double-stranded DNA virus in the Orthopoxvirus genus, transmitted to humans from animals—with symptoms similar to smallpox although clinically less severe. Details about the disease are available on WHO’s website.1
Since early May 2022, cases of monkeypox have been reported in countries where the disease is not endemic and continue to be reported in several endemic countries. Most confirmed cases with travel history reported travel to countries in Europe and North America, rather than West or Central Africa, where the monkeypox virus is endemic. This is the first time that many monkeypox cases and clusters have been reported concurrently in non-endemic and endemic countries in widely disparate geographical areas.2 As of Aug. 8, 30,189 cases have been reported from 88 countries, out of which 29,844 cases are from countries that have not historically reported monkeypox3.
Most reported cases so far have been identified through sexual health or other health services in primary and secondary health care facilities and have involved mainly, but not exclusively, men who have sex with men.
Human infection with monkeypox virus was initially identified in 1970, with almost all subsequent cases confined to rainforest regions of central and west Africa. In Africa, human case fatality rates from monkeypox infection are approximately 10%, and nearly half of infected individuals develop severe complications. In recent times, case fatality rate is around 3% to 6%1.
In the summer of 2003, there was an outbreak of monkeypox virus infection in 72 individuals (34 confirmed cases) in the midwestern United States, the first human infections reported from outside the African continent5. Fifteen percent of the confirmed cases were seriously ill, including one patient with severe encephalitis.
The most common symptoms included rash, fever, chills and/or rigors, adenopathy, headache, myalgia, sweats, and cough. Rash, predominantly centrifugal involving palms and soles, follows the viral-like prodrome after one to three days.
 Neurological manifestations in the form of headache and malaise are observed in more than 50% of patients, while more serious complications like encephalitis and seizures are seen in less than 3% of patients.6 Anxiety and depression are common in hospitalized patients. Two cases of encephalitis due to monkeypox, both in girls requiring intubation and mechanical ventilation, are reported in the literature during past outbreaks7.
Neurological manifestations in the form of headache and malaise are observed in more than 50% of patients, while more serious complications like encephalitis and seizures are seen in less than 3% of patients.6 Anxiety and depression are common in hospitalized patients. Two cases of encephalitis due to monkeypox, both in girls requiring intubation and mechanical ventilation, are reported in the literature during past outbreaks7.
The U.S. patient with monkeypox encephalitis was a 6-year-old girl who initially presented with fever, pharyngitis, anorexia, malaise, and headache and was noted to have adenopathy and a vesiculopapular rash. She subsequently became somnolent and unresponsive and developed presumed seizure activity. Her MRI brain, EEG, and cerebrospinal fluid (CSF) revealed abnormalities. Diagnosis was confirmed by detection of monkeypox virus IgG and IgM in serum and IgM in CSF and by positive culture, immunohistochemical, and PCR results on skin lesion material. The patient gradually improved over several weeks, eventually recovering fully8,4. The other was a 3-year-old girl who died on day 2 of hospitalization but CSF diagnostics were not performed7.
Because IgM does not generally cross the blood-brain barrier, the presence of IgM in CSF indicates active central nervous system infection with intrathecal antibody production. The absence of demyelination, cytotoxic changes caused by diffuse and focal edema, and intrathecal antibodies (IgM) all point to monkeypox as a possible cause of acute encephalitis7.
Monkeypox appears to have a fatal course almost exclusively in infants and young children, specifically those who have not received vaccination against smallpox.
These are early days, and we may find more cases with neurological involvement in the coming weeks or months. Any person with fever, rash, lymphadenopathy, and altered sensorium should be suspected as a case of monkeypox encephalitis. •
Chandrashekhar Meshram is co-opted trustee of the WFN.
References and further reading
- https://www.who.int/news-room/fact-sheets/detail/monkeypox
- https://www.who.int/emergencies/situations/monkeypox-oubreak-2022
- https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html
- Tyler KL emerging viral infections of central nervous system part 2. Arch Neurol 2009:66(9):1065-1074.
- Reed KDMelski JWGraham MB et al. The detection of monkeypox in humans in the Western hemisphere. N Engl J Med 2004;350 (4) 342- 350
- James B Badenoch, Isabella Conti, Emma R Rengasamy, Cameron J Watson, Matt Butler, Zain Hussain, Alasdair G Rooney, Michael S Zandi, Glyn Lewis, Anthony S David, Catherine F Houlihan, Ava Easton, Benedict D Michael, Krutika Kuppalli, Timothy R Nicholson, Thomas A Pollak , Jonathan P Roger Neurological and psychiatric presentations associated with human monkeypox virus infection: a systematic review and meta-analysis medRxiv preprint doi: https://doi.org/10.1101/2022.07.03.22277069
- Caleb RS McEntire, Kun-Wei Song, Robert P McInnis, John Y Rhee, Michael Young, Erica Williams, Leah L Wibecan, Neal Noha, Amanda M Nagy, Jeffrey Gluckstein, Shibani S Mukerji and Farrah J Matin Neurologic Manifestations of the World Health Organization’s List of Pandemic and Epidemic Diseases Front. Neurol., 22nd February 2021 Sec. Neuroinfectious Diseases https://doi.org/10.3389/fneur.2021.634827
- Sejvar JJ, Chowdary Y, Schomogyi M, et al. Human monkeypox infection: a family cluster in the Midwestern United States. J Infect Dis. 2004;190(10):1833-1840.
- Shafaati M, Zandi M. Monkeypox virus neurological manifestations in comparison to other orthopoxviruses Travel Medicine and infectious diseases Volume 49, September October 2022, 102414
 The WFN’s policies regarding industry sponsorship, continuing medical education (CME), and conflicts of interest (COI) are provided here.
The WFN’s policies regarding industry sponsorship, continuing medical education (CME), and conflicts of interest (COI) are provided here. World Brain Day 2022 was celebrated with great fanfare and enthusiasm in India, and the campaign was extended over a week. This year’s theme “Brain Health for All” was appropriate, and it generated a lot of interest. Although the Dynamic President of the Indian Academy of Neurology (IAN) Nirmal Surya had given an ambitious target of 100 activities during the week, we ended up doing many more events across the country. The activities were focused on increasing awareness of common people and students about brain health and neurological diseases.
World Brain Day 2022 was celebrated with great fanfare and enthusiasm in India, and the campaign was extended over a week. This year’s theme “Brain Health for All” was appropriate, and it generated a lot of interest. Although the Dynamic President of the Indian Academy of Neurology (IAN) Nirmal Surya had given an ambitious target of 100 activities during the week, we ended up doing many more events across the country. The activities were focused on increasing awareness of common people and students about brain health and neurological diseases. Man Monahan Mehndiratta, chair, and Abhishek Shrivastava, convener of Neurorehabilitation subsection of IAN, conducted four webinars: Brain Health, Neuroplasticity—Rewiring the Brain, Cognition and Brain Health, and Update on Neuromodulation.
Man Monahan Mehndiratta, chair, and Abhishek Shrivastava, convener of Neurorehabilitation subsection of IAN, conducted four webinars: Brain Health, Neuroplasticity—Rewiring the Brain, Cognition and Brain Health, and Update on Neuromodulation.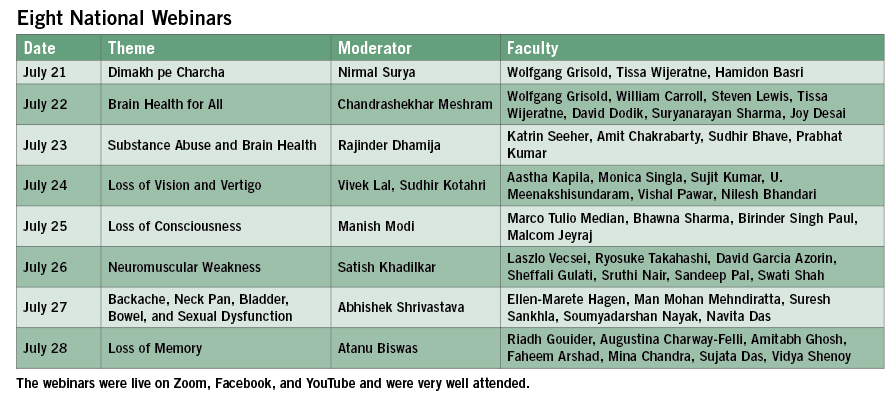 Nagpur—14 Activities Plus 43 Publications
Nagpur—14 Activities Plus 43 Publications  Suvarna Alladi and NIMHANs team organized a cricket match with cricketer Robin Uthappa who is brand ambassador of Karnataka’s brain health initiative. Policymakers, patients, care givers, institutional heads, and neurologists participated in the event. Karnataka Health Minister K. Sudhakar inaugurated the first of its kind brain health clinic in the Bangalore Hospital. It was supported by six newspaper publications. Amit Kulkarni delivered a public talk at Global Institute of Technology. Suryanarayan Sharma gave lectures in two colleges, and also at Toyota Industries. He organized the painting competition for school children. His interview was published in the newspaper and he did two digital platform activities. B. K. Madhusudan gave a talk at the university and had one Facebook live event on brain health.
Suvarna Alladi and NIMHANs team organized a cricket match with cricketer Robin Uthappa who is brand ambassador of Karnataka’s brain health initiative. Policymakers, patients, care givers, institutional heads, and neurologists participated in the event. Karnataka Health Minister K. Sudhakar inaugurated the first of its kind brain health clinic in the Bangalore Hospital. It was supported by six newspaper publications. Amit Kulkarni delivered a public talk at Global Institute of Technology. Suryanarayan Sharma gave lectures in two colleges, and also at Toyota Industries. He organized the painting competition for school children. His interview was published in the newspaper and he did two digital platform activities. B. K. Madhusudan gave a talk at the university and had one Facebook live event on brain health.






 The WFN/AAN Continuum program for low- and lower-middle-income countries occurs through the generous donation of 400 print copies of each issue of Continuum from the AAN and its publisher, Wolters-Kluwer, while also providing online access to issues. The program allows access for continuing education and self-assessment, point-of-care use, as well as use in Continuum user groups where the content is used as the basis for joint educational activities. Now being distributed to 49 countries worldwide, this important educational resource has been integral in the education and continued education for neurologists worldwide. Continuum user groups have included in-person and (increasingly) virtual meetings, using the material in each issue as a source of content for presentations and group discussions.
The WFN/AAN Continuum program for low- and lower-middle-income countries occurs through the generous donation of 400 print copies of each issue of Continuum from the AAN and its publisher, Wolters-Kluwer, while also providing online access to issues. The program allows access for continuing education and self-assessment, point-of-care use, as well as use in Continuum user groups where the content is used as the basis for joint educational activities. Now being distributed to 49 countries worldwide, this important educational resource has been integral in the education and continued education for neurologists worldwide. Continuum user groups have included in-person and (increasingly) virtual meetings, using the material in each issue as a source of content for presentations and group discussions. Given the importance of Continuum in worldwide neurology education, and in particular the continued education of neurologists in low- and lower-middle-income countries, the WFN has now created a Continuum subcommittee of the Education Committee, consisting of members from the AAN Continuum editorial office and members of the WFN executive leadership. This will enable enhanced mutual collaboration to continue to optimize the program’s evolution for the purpose of ensuring that this vital resource is available and utilized as optimally as possible globally.
Given the importance of Continuum in worldwide neurology education, and in particular the continued education of neurologists in low- and lower-middle-income countries, the WFN has now created a Continuum subcommittee of the Education Committee, consisting of members from the AAN Continuum editorial office and members of the WFN executive leadership. This will enable enhanced mutual collaboration to continue to optimize the program’s evolution for the purpose of ensuring that this vital resource is available and utilized as optimally as possible globally. Continuum is committed to diversity, including within its editorial board as well as in the selection of guest editors and in the selection of content experts to write articles for each issue. All authors for Continuum are instructed to include relevant information in each article about health care inequities and disparities and some issues have even begun to incorporate entire articles devoted to this critically important topic1.
Continuum is committed to diversity, including within its editorial board as well as in the selection of guest editors and in the selection of content experts to write articles for each issue. All authors for Continuum are instructed to include relevant information in each article about health care inequities and disparities and some issues have even begun to incorporate entire articles devoted to this critically important topic1. We are pleased that this vital resource has been so well received and used by so many neurologists (and trainees) worldwide. We look forward to continuing to provide this important educational journal to neurologists in low- and lower-middle-income countries and look forward to hearing from neurologists to learn of any ways that we can enhance this program for the goal of providing the most up-to-date information to neurologists throughout the world. •
We are pleased that this vital resource has been so well received and used by so many neurologists (and trainees) worldwide. We look forward to continuing to provide this important educational journal to neurologists in low- and lower-middle-income countries and look forward to hearing from neurologists to learn of any ways that we can enhance this program for the goal of providing the most up-to-date information to neurologists throughout the world. • Steven Lewis is acting secretary general of the WFN, editor-in-chief of Continuum: Lifelong Learning in Neurology, and editor of World Neurology. Andrea Weiss is executive editor for Education and News Publications for the AAN.
Steven Lewis is acting secretary general of the WFN, editor-in-chief of Continuum: Lifelong Learning in Neurology, and editor of World Neurology. Andrea Weiss is executive editor for Education and News Publications for the AAN.







