The WHO calls for global action plan to combat epilepsy and other neurologic disorders
By William Carroll
As we reach the end of a very trying year with COVID-19 still rampant, I have two pieces of good news, in some respects, as good as the imminent arrival of the vaccines.
The first is a momentous decision by the WHO and the second is an important and rewarding development for the WFN. Both point us all in the same direction.

William Carroll, MD
The decision by the World Health Assembly (WHA) on Nov. 12, 2020, to adopt Resolution WHA73.10 is a landmark event. Although the WFN has been closely involved with neurological activities within, and related to, the WHO, the call for the development of global action plans to combat epilepsy and (importantly) neurological disorders, is a first. It comes courtesy of a sustained effort by the ILAE (led recently by Prof. Sam Wiebe) and International Bureau for Epilepsy (IBE) to convince the WHO that epilepsy is a common disease, causing considerable effect upon people, their neurological health, their cognitive function, societal burden, and individual stigmatization for want of the ready availability of anticonvulsant medication.
William Carroll, MDIt also occurred through the recognition of certain key member states that saw the synergies between the dilemma of epilepsy and those suffering from it, with a number of other important neurological processes. The resulting WHA73.10 Resolution was carried unanimously by members of the 74th Executive Board and thence the 73rd World Health Assembly. In Clause (PP2) of WHA73, it is clear that the authors and the supporting member states recognized a need to address all neurological disorders. The clause specifically mentions epilepsy, headache disorders, neurodevelopmental, neurodegenerative, neuroinfectious/neuroimmunological, cerebrovascular diseases including stroke, and traumatic brain and spinal cord disorders. There is scarcely a single neurological disorder not encompassed by this regulation. (See below.)
The regulation seeks to develop a comprehensive intersectoral approach to addressing all neurological disorders in line with the third pillar of the U.N. Sustainable Development Goals.
For the first time, neurological disorders are being overtly recognized for the threat they pose to all societies and health jurisdictions. We need look no further than the most recent Global Burden of Disease Study, which demonstrated neurological non-communicable disorders to be the leading cause of disability and the second leading cause of death. To have the WHO acknowledge the need for global action plans to address this burden will provide enormous assistance to those at risk of neurological disorders and those attempting to combat them.
The WFN was proud to lend its support to the ILAE and IBE at the WHA71 (May 2018) “Side Event for Global Action on Epilepsy” and a statement calling for a new report on the implementation of Resolution WHA68.20 to be prepared for discussion at the WHA74 meeting in 2021.

Photo of WHA 73 from the WHO website.]
At the 144th Executive Board Meeting in January/February 2019, the WFN posted a statement asking the EB not to defer consideration on further actions to address the global burden of epilepsy and its health and social implications at the country level. Again, in May 2019, we joined with the ILAE and IBE to support this initiative in a further Side Event, urging member states to implement a coordinated action against epilepsy through the establishment of:
- national Health Care Plans for epilepsy management to overcome inequalities and inequities in health, social, and other related services
- initiatives to promote public awareness of an education about epilepsy, and to reduce the misconceptions, stigmatization and discrimination against people with epilepsy
- actions to prevent causes of epilepsy
- greater investment in epilepsy research and increased research capacity.
The WFN also posted a statement on the Prevention and Control of Non-Communicable Diseases (Agenda item 11.8) highlighting the need to:
- elucidate treatments to prevent and/or modify stroke, migraine, and Alzheimer’s Disease and other dementias
- the disparity between high and low sociodemographic index nations and the resultant unequal burden on resources
- that the WFN was uniquely placed as the only global neurological organization with an almost identical matching regional and national reach.
The statement pointed to the WFN’s geographical advantage in advocacy partnership being bolstered by its relationship with associated disease topic organizations of the Global Neurological Alliance, such as the World Stroke Organization, Alzheimer’s Disease International, Parkinson’s Disease and Movement Disorders Society, the International League Against Epilepsy, and Multiple Sclerosis International Federation.
At the 146th Executive Board meeting in February 2020, the WFN supported the draft decision on the 2019 Global Report “Epilepsy as a Public Health Imperative” proposed by the Russian Federation and co-sponsored by China and Guyana. The WFN statement also requested the WHO director-general to expand the scope of the report EB146/12 to be presented at the 73rd WHA with an additional consideration of “Synergies in Addressing the Burden of Epilepsy and Other Neurological Disorders” and among other calls “to encourage member states and related non-state actors to contribute to discussions” on the “draft resolution on epilepsy and other neurological disorders” based on the report mentioned in paragraph 2 to be presented for consideration by the 73rd WHA.
The leadership demonstrated by the WHO in the adoption of WHA73.10 will be of inestimable benefit in the energization of all those faced with combating neurological disorders, particularly non-communicable neurological disorders and their devastating effect on individuals and societies. For those so engaged to know that the WHO, through its member states, will be encouraging, advocating, and leading the intersectoral struggle will be heartened.
There will be many non-state actors, such as the WFN, that will be similarly buoyed. To address these challenges in the manner outlined in the WHA73.10 Resolution will also require the development and implementation of plans to overcome many barriers, which have contributed to the inequities of access most keenly felt by less well-resourced jurisdictions. The leadership of the WHO will be pivotal in maintaining the momentum required.
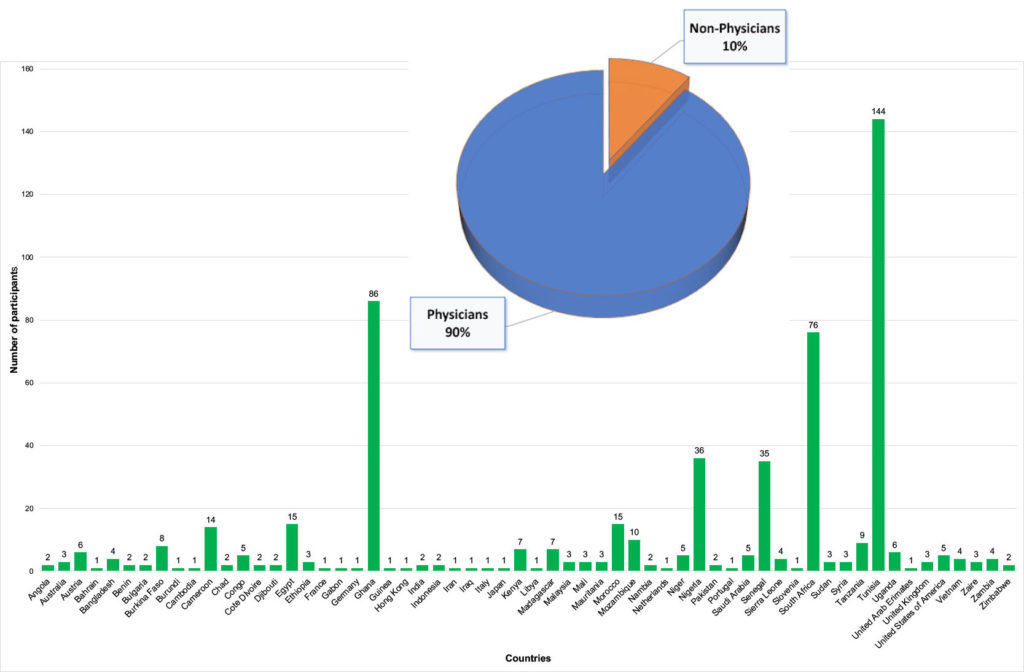
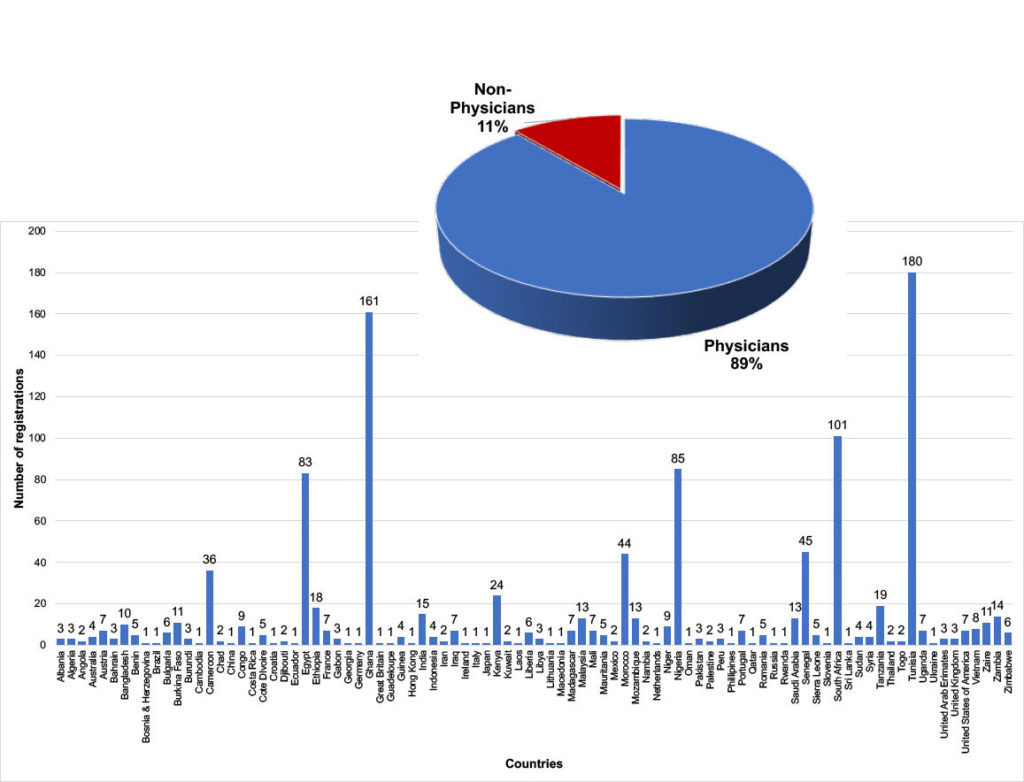
Finally, this most welcome event sits closely with the WFN Needs Registry. This registry was conceived to provide a complementary balance to the data supplied by WHO member states. Member states are by and large national governments. The WFN Needs Registry is the product of WFN member societies, which are in turn composed of neurologists and allied neurological colleagues on whom people with neurological disease depend for prevention, diagnosis, and treatment. The data collected by the Needs Registry offers opportunities to advocate for the redirection of resources as well as additional resources where possible and to do so collectively with member societies and jurisdictions sharing common challenges.
Given the position of the WFN and its relationship with the Global Neurology Alliance and the World Health Organization, it is likely to be able to contribute considerably to the attainment of useful outcomes in line with WHA73.10. In this regard, the WFN is planning to discuss in 2021 with each of its regional organizations ways in which these processes might be advanced.
I wish you your families and colleagues a safe and joyous time through the festive season and a better New Year for all. •
The 73rd World Health Assembly Resolution WHA73.10
(PP1) Recognizing that epilepsy and other neurological disorders are the leading cause of disability-adjusted life years and the second leading cause of death worldwide, and that epilepsy and other neurological disorders disproportionately impact people living in low- and middle-income countries;1
(PP2) Noting that neurological disorders are conditions of the central and peripheral nervous system that include epilepsy, headache disorders, neurodegenerative disorders, cerebrovascular diseases including stroke, neuroinfectious/neuroimmunological disorders, neurodevelopmental disorders and traumatic brain and spinal cord injuries;2
(PP3) Noting with concern that the risk of premature death in people with epilepsy is three times higher than in the general population and that, over the past 30 years, the absolute number of deaths due to neurological disorders has increased by 39%;3
(PP4) Acknowledging, as outlined in the WHO/ International League Against Epilepsy/International Bureau for Epilepsy Global Report on Epilepsy (2019), that epilepsy is one of the most common neurological disorders globally affecting an estimated 50 million people worldwide across all ages with increased rates in the young and the old…
(OP1) URGES Member States:1
(OP 1.1) To provide the appropriate support to WHO to develop the Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders referenced in paragraph 3.1;
(OP2) CALLS UPON all relevant stakeholders:
(OP2.1) To provide appropriate support to WHO and partners to develop the Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders referenced in paragraph 3.1;
(OP3) REQUESTS the Director-General:
(OP3.1) To develop, in consultation with Member States, and in full collaboration with United Nations organizations and relevant non-State actors, a 10-year Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders in support of universal health coverage to address the current significant gaps in promotion of physical and mental health, and prevention, early detection, care, treatment and rehabilitation, as well as social, economic, educational and inclusion needs of persons and families living with epilepsy and other neurological disorders, and the ongoing need for research to improve prevention, early detection, treatment, care and rehabilitation, including treatment options with the potential to cure epilepsy and other neurological disorders;
(OP3.2) To include in the Intersectoral Global Action Plan ambitious, but achievable, global targets on reducing preventable cases of, and avoidable deaths, resulting from epilepsy and other neurological disorders, strengthening service coverage and access to essential medicines, improving surveillance and critical research and addressing discrimination and stigma;
(OP3.3) To submit to the 150th Executive Board, a draft Intersectoral Global Action Plan for consideration by Member States, as well as to report on the progress achieved in implementing this resolution, with an intention to submit the plan to Member States for endorsement during the 75th World Health Assembly. •





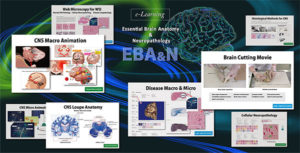 EBA&N consists of various whole slide images (Cellular Neuropathology, Disease Cytopathology, Normal Histopathology, Muscle Diseases), in addition to brain cutting videos and many photographs. It is very easy to understand because the commentary is written directly on the images and videos, not as footnotes.
EBA&N consists of various whole slide images (Cellular Neuropathology, Disease Cytopathology, Normal Histopathology, Muscle Diseases), in addition to brain cutting videos and many photographs. It is very easy to understand because the commentary is written directly on the images and videos, not as footnotes.




 During this stay, I had the opportunity to make daily visits to patients in the neurology department and also to participate in the outpatient consultation where I had the chance to strengthen my skills in the diagnosis and management of neurological pathologies, more specifically epilepsy. I also experienced a number of neurodegenerative and autoimmune pathologies, such as multiple sclerosis, amyotrophic lateral sclerosis, and severe myasthenia gravis.
During this stay, I had the opportunity to make daily visits to patients in the neurology department and also to participate in the outpatient consultation where I had the chance to strengthen my skills in the diagnosis and management of neurological pathologies, more specifically epilepsy. I also experienced a number of neurodegenerative and autoimmune pathologies, such as multiple sclerosis, amyotrophic lateral sclerosis, and severe myasthenia gravis.
 The World Federation of Neurology (WFN) and the African Academy of Neurology presented their first virtual one-day teaching course—the first WFN/AFAN e-Learning Day—which took place from 8:45 a.m. to 6 p.m. (BST), Saturday, Oct. 10, 2020.
The World Federation of Neurology (WFN) and the African Academy of Neurology presented their first virtual one-day teaching course—the first WFN/AFAN e-Learning Day—which took place from 8:45 a.m. to 6 p.m. (BST), Saturday, Oct. 10, 2020.