Raad Shakir
Over the last three months, the world has been facing a most serious and devastating epidemic. The World Health Organization (WHO) declared Zika virus infection as a Public Health Emergency of International Concern (PHEIC). This has triggered a massive international response not only in the Americas, but also across the world. Cases of Zika virus infection are being reported in the thousands across the northern parts of South and Central America. To date, the WHO reports the infection to be present in 62 countries between 2007 and 2016. The transmission is not only reported in Latin America, but in Cape Verde, and recently Vietnam reported mosquito-borne Zika virus infection.
The issue is compounded by the fact that the symptoms of the Zika virus infection are mild, and none disabling. However, the neurological complications are most serious. Zika virus infection is described as the most devastating viral infection during pregnancy. The reported microcephaly is most serious, and we have no idea what the future holds for those babies born to mothers without obvious microcephaly. One can reasonably conclude that the reported Zika virus isolated from post mortem cases of invasion of brain and spinal cord suggests that we may be facing a future group of affected children with many neurological complications of as yet unknown nature.

Figure 2- left to right, Dr. Iledefonso Rodriguez Leyva, Dr. Karina Velez Jimenez, Professor Raad Shakir, Dr. Minerva Lopez, Dr. Steven L. Lewis, during the WFN visit to neurology training programs in Mexico City.
The second neurological condition which has increased in those affected with Zika virus infection is Guillain-Barre syndrome. This, in a way, is expected following a viral infection. The seriousness of the condition is made much worse by the lack of local availability of supportive treatment. Generally, at least a fifth of GBS patients may require respiratory support, which is compounded with lack of availability of IV immunoglobulin. The cost of both modalities is prohibitive. In some parts of Latin America, the use of plasma exchange is the way GBS is treated rather than IV immunoglobulin. Even with this, many locations in affected areas do not have the facilities or the training to use plasma exchange machines. This puts lives at risk.
One has to remember that the diagnosis and management of GBS requires neurological expertise, which is scarce to say the least. It would be reasonable to state that the 1 in 20 mortality rate reported in the developed world will be much higher for those affected by GBS in the currently Zika virus affected areas.
All this prompted the WFN to mount a concerted effort to tackle the problem. The WFN Zika Virus Working Group was formed, and the committee is chaired by John England, MD, New Orleans. The membership includes experts in child neurology and GBS, with neurologists from the most affected countries in South and Central America. See more at www.wfneurology.org/committees?tab=16016.

Meeting of the WFN with some of the members of the Zika Working Group at the American Academy of Neurology Annual Meeting April 18 in Vancouver. From left to right: Raad Shakir, MD; David Bearden MD; Ildefonso Rodriguez-Leyva, MD; Miguel Osorno Guerra, MD; Minerva Lopez Ruiz, MD; Karina Velez Jimenez, MD; Allen Aksamit, MD; and Russell Bartt, MD; Also participating in the meeting, but not in the photo, were William Carroll, MD, Wolfgang Grisold, MD, Steven Lewis, MD, and Marco T. Medina, MD.
Meeting of the WFN with some of the members of the Zika Working Group at the American Academy of Neurology Annual Meeting April 18 in Vancouver. Meeting of the WFN with some of the members of the Zika Working Group at the American Academy of Neurology Annual Meeting April 18 in Vancouver.
The WFN is also an active contributor to the WHO committee on Zika. This committee met in Geneva, and according to Dr. England’s executive summary, “Collaborative interdisciplinary research on Zika infection and its neurological complications is already being organized, but funding is severely lacking at this time. As an important first step to enhance research collaboration and provide for transparent data sharing, the Neurovirus Emerging in the Americas Study (NEAS), www.neasstudy.org/en/home/, is being organized and is supported by an approved Johns Hopkins Medical Institutions IRB protocol. Researchers are encouraged to visit the NEAS website for additional information. The situation is rapidly evolving; therefore, all information is subject to modification as we learn more about this emerging crisis.”
The WHO situation report on April 7, 2016 concludes “The global prevention and control strategy launched by the World Health Organization (WHO) as a Strategic Response Framework encompasses surveillance, response activities, and research. This situation report is organized under those headings.”
The WFN Zika virus committee met on Monday, April 18th in Vancouver during the 68th AAN meeting to further discuss the issues. The following questions were put to the experts for a response.
- Do we have a diagnostic ELISA test or the like, for quick diagnosis?
- Can individuals have the neurological complications without exhibiting the febrile illness, and if so how can we be sure of diagnosis?
- Do we know the spectrum of all the fetal neurological deficits?
- How long is the period of viral human-to-human infectivity after the Zika virus infection illness?
- Do we have a registry of morbidity and mortality related to GBS resulting from Zika virus infection?
- It is important to understand whether the variant of GBS associated with Zika is different than other varieties of GBS.
- Is there a registry of cases of neurological Zika virus infection other than GBS?
- Any report on vaccine development?
- Is Zika virus present in breast milk and what is the risk to breast-fed infants?
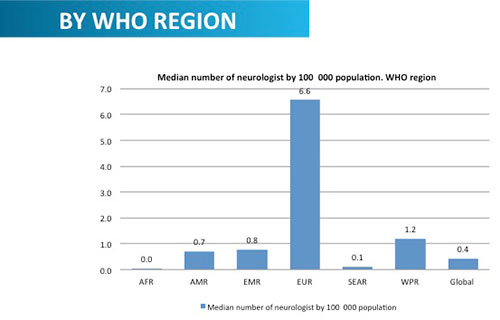
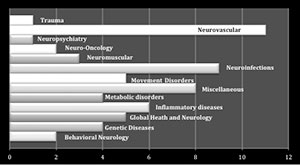
Legend Fig. 1 Neurology Atlas 2015. Editor’s note: The data in the Neurology Atlas figure are a draft and the definitive data may be different when the final WHO version is produced.
One can easily see that the brunt of the neurological complications fall in the child neurology world. The WFN is working very closely with the International Child Neurology Association to collaborate and come up with a joint stance in combating this most devastating viral infection during pregnancy. The ICNA is dedicating a session of its forthcoming world congress to Zika viral infection.
The division of mental health, substance abuse, and neurosciences in the WHO is very keen on informing member states on the importance of neurological expertise in the fight against Zika virus infection. This has brought into focus the dire lack of neurologists both for adults and children across the world. The second edition of the Neurology Atlas jointly produced by the WHO and the WFN has demonstrated in its figures that the mean number of neurologists per 100,000 people is 0.7 in the Americas, compared to 6.6 in Europe (Fig1). The figures are more poignant as the Pan American region includes the U.S. and Canada. The logical conclusion is that there is a vast shortage in the areas affected by Zika virus infection.
The WFN is collaborating with the Canadian Neurological Society to join the worldwide program for short-term training of young neurologists and in this case neurologists will be chosen from Latin America for short training periods in Canada. The WFN has already had such a program with four European countries for training African Neurologists, and now the program is branching out to the Americas.
In March 2016, the neurology training program in Mexico has been inspected and accredited by the WFN, and a similar short-term training will start. Mexico already trains young neurologists from across Central America (Fig2).
Perhaps Zika virus infection has produced a momentum for all of us to demonstrate our willingness to cooperate and act quickly in the face of this pandemic. We are at the beginning of a long, difficult, and tortuous road.
 The global share of older people (age 60 and over) is more than 800 million (12 percent of the population) and is growing, with the expectation that it will reach more than two billion (21 percent of the population) by 2050. Currently 70 percent of the world’s older population lives in developed and developing countries, but by 2025, 80 percent of the older population will be living in less developed countries. Older persons are projected to exceed the number of children in 2047. It has already started in developed countries. In 2015, Japan became the first country in the world where more adult diapers than baby diapers were sold.
The global share of older people (age 60 and over) is more than 800 million (12 percent of the population) and is growing, with the expectation that it will reach more than two billion (21 percent of the population) by 2050. Currently 70 percent of the world’s older population lives in developed and developing countries, but by 2025, 80 percent of the older population will be living in less developed countries. Older persons are projected to exceed the number of children in 2047. It has already started in developed countries. In 2015, Japan became the first country in the world where more adult diapers than baby diapers were sold.










 1) Ivana Vodopivec, et al. provides a glimpse of the heterogeneity of patients with Susac syndrome. Susac syndrome is a rare disease, which is usually characterized by a triad of encephalopathy, visual disturbances and hearing loss attributed to a pauci-inflammatory vasculopathy of the brain, eye and inner ear. However, at initial presentation, none of the five patients in this case series demonstrated the complete triad, and diagnosis was difficult and delayed. The authors provide two important conclusions: a) Microinfarcts were noted on MRI diffusion weighted imaging (DWI) of the brain, as well as branch retinal artery occlusions and vessel wall hyperfluorescence on fluorescein angiography in all patients with acute encephalopathy, and b) glucocorticoid and IVIg treatments were insufficient in halting the disease in patients with severe encephalopathy. Additional immunosuppressive treatment was required.
1) Ivana Vodopivec, et al. provides a glimpse of the heterogeneity of patients with Susac syndrome. Susac syndrome is a rare disease, which is usually characterized by a triad of encephalopathy, visual disturbances and hearing loss attributed to a pauci-inflammatory vasculopathy of the brain, eye and inner ear. However, at initial presentation, none of the five patients in this case series demonstrated the complete triad, and diagnosis was difficult and delayed. The authors provide two important conclusions: a) Microinfarcts were noted on MRI diffusion weighted imaging (DWI) of the brain, as well as branch retinal artery occlusions and vessel wall hyperfluorescence on fluorescein angiography in all patients with acute encephalopathy, and b) glucocorticoid and IVIg treatments were insufficient in halting the disease in patients with severe encephalopathy. Additional immunosuppressive treatment was required.


 Although ancient Egyptians were the first to describe the brain, the services that are provided to patients with disorders of the brain and the number of trained neurologists in Arab and African countries is at best centralized in large cities and at worst nonexistent.
Although ancient Egyptians were the first to describe the brain, the services that are provided to patients with disorders of the brain and the number of trained neurologists in Arab and African countries is at best centralized in large cities and at worst nonexistent.
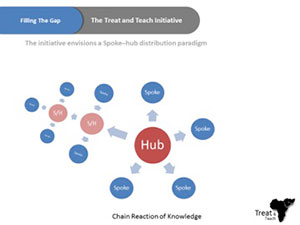 For the aforementioned reasons, Ain Shams University has been endorsing an initiative called Treat and Teach, which is designed to develop short- and intermediate-term strategies to reduce the gap in the number of trained neurologists and the deficiency of neurology education programs in Africa. We are trying to complement the current efforts to improve neurology education in Africa with an initiative that has a mix of online education and on-site clinical training, while working on establishing medical services that may include a stroke unit, memory clinic, neurorehabilitation units, or a neurology department. Master degrees will be given from Ain Shams University, Cairo, and work will be done to establish local master degrees in rural centers. This could lead to national neuroscience services run by local providers.
For the aforementioned reasons, Ain Shams University has been endorsing an initiative called Treat and Teach, which is designed to develop short- and intermediate-term strategies to reduce the gap in the number of trained neurologists and the deficiency of neurology education programs in Africa. We are trying to complement the current efforts to improve neurology education in Africa with an initiative that has a mix of online education and on-site clinical training, while working on establishing medical services that may include a stroke unit, memory clinic, neurorehabilitation units, or a neurology department. Master degrees will be given from Ain Shams University, Cairo, and work will be done to establish local master degrees in rural centers. This could lead to national neuroscience services run by local providers.