By Wolfgang Grisold
An international conference, focusing on “multidisciplinary strategies to prevent and combat brain diseases,” took place in Moscow on November 27-28, 2019, and followed the concept of integration and multidisciplinarity. The organization was smoothly run by Prof. Alla Guekht and her team and linked neurology to neurosurgery, internal medicine, and psychiatry. The meeting was held in the Buyanov’s city hospital, and needless to say was equipped with all facilities, including press briefings before the meeting.
Wolfgang Grisold
The opening ceremony gave greetings from the Russian health care minister, Veronica Skvortsova, the Moscow head of the health care department, Alexey Khripun, the president of the All-Russian Society of Neurologists, Y.I. Gusev, and from the leading international neurological organizations — WFN, EAN, and ELAE. A short presentation about the WFN activities in regard to education, global networks, and cooperation with the WHO was made.
Dr. J. Breda, as the chair of the European regional NCD bureau of WHO, gave an initial presentation on the work of the WHO, primary care, and also aspects of environment and nutrition, which are eminently important for many non-communicable diseases (NCDs). This talk and statements are important for the mutual understanding of the specialization of neurology and the activities of the WFN. This was followed by a talk focusing on the historic role of Russian neurology. The impressive figure of the beginning of the 20th century, Bekhterev, was discussed, including his longing for innovation and his successful achievements in neurology, psychiatry, and health care organization and education.

Opening ceremony
From left to right: Prof. M .Hilz (Germany), Prof. D. Muresanu (Romania), V.N. Buzin (Ministry of Health of the Russian Federation), Prof. A.B.Guekht (Russia), Dr. J.Breda (Portugal), Prof. W. Grisold (Austria), Prof. N.A. Shamalov (Russia), Dr. A.V.Salikov (Russia).
During the first day of the conference, several other topics, such as stroke, rehabilitation, the autonomic nervous system, and neurooncology, were presented. Although these topics have defined contents being discussed at many occasions, the keynote speakers were able to pick out exciting developments and add valuable information.

J. Breda, the head of the European Office for the Prevention and Control of Noncommunicable Diseases (NCDs) in Moscow.
The second day entered the often-neglected chapter of neuropsychiatry, which reemerges in international fields and undergoes a metamorphosis from conversion into functional disorders. This lecture by Prof. W. Curt LaFrance Jr. (U.S.) made two important points: functional disorders exist and may be more frequent than we admit, and several concepts of explanation and treatment were available. Another message was that a society for functional disorders has been recently established.
A complex of lectures discussed epilepsy and seizures. Epidemiology and the complex meaning of incidence and prevalence were beautifully and carefully explained by Prof. W. Allen Hauser (U.S.), who shared his insights into this important basis of his work and considerations. Several other lectures addressed epilepsy and seizures, and were supported by excellent videos of patients, EEG recordings, and imaging.

Prof. Hilz and Prof. Mkrtchan discussing the study on autonomic dysfunction in epilepsy.
The end of the second day was devoted to carefully prepared case presentations, which focused on several topics, such as complicated cerebrovascular disease, genetic diseases, complex seizures, neuroinfections, and rare neuropathies. In several cases, speakers from other disciplines were invited to make valuable comments and give diagnostic clues. The spirit of these case presentations was enthusiastic and also made it clear that neurology is deeply rooted in multidisciplinary and multiprofessional work. From the engagement of speakers and the audience, these short case presentations seemed to become a well-accepted format.

Advisory board meeting: Prof. A. Guekht presenting the achievements of the Moscow Research and Clinical Center for Neuropsychiatry.
On the third day, there was a meeting in the Moscow Research and Clinical Center for Neuropsychiatry within the international advisory board of the center. The members of international and Russian faculty discussed ongoing collaborative projects on comorbidity of epilepsy and mental disorders, self-harm behavior, the role of neuroinflammation in stress, and some others. Junior researchers of the center presented their papers and interesting cases.
Research labs and clinical facilities of the center were presented. The members of the board appreciated the high level of the technologies in the labs and the clinical wards of the center.
The size and the spirit of the meeting also allowed many personal and professional interactions, and faculty members interacted with local neurologists, allowing the platform for advice and cooperation to continue.
Having attended these meetings for brain diseases for several years, the interaction of attendees with the faculty is increasing, the magnitude of interaction and discussion during the meeting is developing, and the impression is that young neurologists and psychiatrists are increasingly fluent in English, which helps increase cooperation and communication. These types of integrative meetings, with a strong educational accent, are valuable not only from the point of content, but also from communication.
Wolfgang Grisold is Secretary General of the WFN.
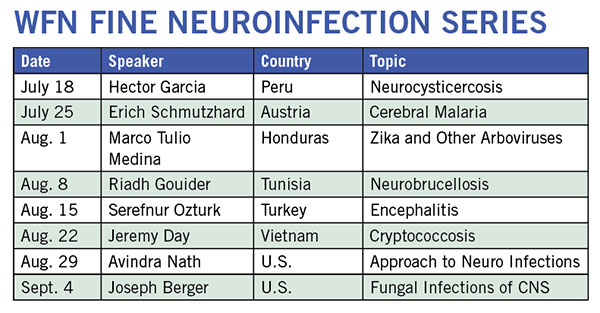




 The World Federation of Neurology and the African Academy of Neurology are delighted to announce to you their first virtual one-day teaching course, the WFN/AFAN e-Learning Day, which will be held on Saturday, October 10, 2020.
The World Federation of Neurology and the African Academy of Neurology are delighted to announce to you their first virtual one-day teaching course, the WFN/AFAN e-Learning Day, which will be held on Saturday, October 10, 2020.

 This is the most important event in the last century. Arguably, aside from the tragic loss of life, the widespread and virtually simultaneous shutdown of global and regional economies, and the restriction of individual movements and travel with the enforcement of social distancing has no precedent. Wars, nuclear bombs, AIDS, global financial crises, and the threat of global warming have not done so much, so rapidly, to so many. Countries, governments, peoples, and individuals are all learning, some the hard way, that without methods to prevent the mutation of new zoonotic viruses and vaccines to combat them, public health measures are all we have to reduce the toll of human lives and the economic consequences which, in turn, also impact human life and livelihoods. The constraints effected by the implementation of public health restrictions and the unparalleled rise in the use and need for health, hospital, and ICU resources affects all aspects of health care globally and at all levels of socioeconomic standing.
This is the most important event in the last century. Arguably, aside from the tragic loss of life, the widespread and virtually simultaneous shutdown of global and regional economies, and the restriction of individual movements and travel with the enforcement of social distancing has no precedent. Wars, nuclear bombs, AIDS, global financial crises, and the threat of global warming have not done so much, so rapidly, to so many. Countries, governments, peoples, and individuals are all learning, some the hard way, that without methods to prevent the mutation of new zoonotic viruses and vaccines to combat them, public health measures are all we have to reduce the toll of human lives and the economic consequences which, in turn, also impact human life and livelihoods. The constraints effected by the implementation of public health restrictions and the unparalleled rise in the use and need for health, hospital, and ICU resources affects all aspects of health care globally and at all levels of socioeconomic standing.
