By Gagandeep Singh, MV Padma, Pramod Pal, Jeyaraj Pandian, PN Sylaja, Suvarna Alladi, and Lalit Dandona

Gagandeep Singh
The burden of neurological diseases as measured by disability adjusted life years (DALYs) and years of life lost is an invaluable piece of information for many. Among the many are health care policy makers, academic institutions, and neurological health care providers. The India State-Level Disease Burden Initiative recently published trends of the burden of neurological diseases across the states of India from 1990 to 20191.
India is seventh largest in terms of area among all countries in the world. It has a population of nearly 1.4 billion, second highest after China, and is slated to be the most populous nation in the world by 2025. The country is geographically divided into 28 states and eight union territories. The per capita gross domestic product of India is US$ 2,100, with a ten-fold variation between the states and union territories. Arguably, therefore, considerable variation is expected in terms of socio-demographic standings, income, and cultural and ecological characteristics between the states of India. Inherent, e.g., genetic, differences are also likely to exist between different subpopulations within the country. Predictably, therefore, disease burdens including those of neurological disorders are likely to vary across the states.
The neurological diseases burden across the states of India, 1990-2019, not only underscores the geographical disparities across India but also the temporal trends in the burden of all neurological diseases combined and a range of neurological disorders1. Overall, neurological disorders accounted for nearly a tenth of DALYs for all diseases combined in India. This proportion increased somewhat between 1990 and 2019; from 8.3% to 9.9%. Remarkably, however, over the same time period, the point estimate of the contribution of non-communicable neurological disorders to DALYs from all causes increased from 4.0% to 8.2%, i.e., doubled.
As distinct from this trend, the proportion of communicable neurological disorders including meningitis, encephalitis and tetanus decreased from 4.1% to 1.1%, i.e., nearly four times. Aside from these two major subgroups of neurological disorders, the contribution of injury-related neurological disorders increased from 0.2% to 0.6%, representing a three-fold increase.
These data are testimony to the epidemiological transition taking place in the country. Over the decades since the Indian independence in 1947, it was assumed that communicable disorders, meaning thereby neurological infections, were the major predicament for Indian health care policy makers and care providers. This is changing and we need to be mindful of this evolution. The increase in injury related DALYs, likely a reflection of increasing use of vehicular transport, is also concerning as it is a largely preventable cause of enormous neurological morbidity and mortality.
The considerable variation in the neurological burden and of the incidence or prevalence and DALYs attributed thereof between the states of India is relevant as health is a state subject in India. Individual states, henceforth, need to prioritize their health care budgets, programmatic undertakings, and health care personnel training slots according to these data. The DALYs of communicable neurological disorders correlate inversely and those of injury-related neurological disorders varied directly with socio-demographic development indices of various states, while there is no such correlation in the case of non-communicable disorders. Subnational or within-country variations in the neurological burden are perhaps relevant to low- and middle-income countries and among them, for the most part to countries with large land areas with multi-ethnic populations, for instance, India and China. In China, likewise, there are remarkable socio-demographic variations between the industrialized east and the agrarian west and these may plausibly impact disease burdens and health care.
How does the neurological disease burden data from India compare with global numbers and proportions? Globally, the top five neurological disorders in terms of proportional contribution are stroke, migraine, Alzheimer’s and other dementias, meningitis, and epilepsy in that order2. Distinct from this, the order in India is as follows: stroke, migraine, epilepsy, cerebral palsy, and encephalitis (Alzheimer’s and other dementias and traumatic brain injuries closely follow encephalitis).
Encouraging to note, the incidence of, and age-standardized DALYs due to, stroke have somewhat declined between 1990 and 2019. This may reflect better preventative care implementation, leading to a reduced incidence and improved treatments in the form of specialist stroke units across the country. The age-standardized point estimates for the prevalence of epilepsies, cerebral palsy, Parkinson’s disease, multiple sclerosis and motor neuron disease have increased markedly. This probably could be attributed to a closing diagnostic gap but also, in case of epilepsies and Parkinson’s disease, increased longevity of the Indian population with time.
In comparison, the increase in prevalence for Alzheimer’s and other dementias is relatively modest, indicating perhaps that a considerable diagnostic gap still exists for this disorder. Inconsistent with the increase in prevalence of epilepsies and Parkinson’s disease, the age-standardized DALY rates attributed to these two neurological disorders have decreased over the past three decades. These surely signal progress in terms of closing the huge treatment gap and improved awareness for the two disorders.
Taken as a whole, the burden of neurological diseases across the states of India provides new information, which is both concerning and reassuring. These data call for a different level of preparedness to respond to the neurological disease burden in India. Moreover, the data call to attention subnational variations, and hence, should be a worthwhile exercise for neurological and epidemiological experts collectively in different nations constituting the membership of the World Federation of Neurology. •
References
- India State-Level Disease Burden Initiative Neurological Disorders Collaborators. The burden of neurological disorders across the states of India: the Global Burden of Disease Study 1990-2019. Lancet Glob Health. 2021 Aug;9(8):e1129-e1144. doi: 10.1016/S2214-109X(21)00164-9.
- GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019 May;18(5):459-480. doi: 10.1016/S1474-4422(18)30499-X.
Gagandeep Singh, MD, DM, FAMS, FRCP is Professor & Head, Department of Neurology Dayanand Medical College Ludhiana, India & Hon. Assoc. Professor Department of Clinical & Experimental Epilepsy Institute of Neurology Queen Square, London.
 Over this past year, we have all come to wonder what we can do to make a difference in the face of problems that seem so overwhelming. When we think about the scope of the pandemic and other global health issues, the devastating numbers are heart breaking, and it’s easy to lose sight of the individual people and stories behind the statistics. In Aaron Berkowitz’s new book, “One by One by One,” he shares with us the lessons he learned as he tried to make a small difference by helping one individual at a time amid suffering measured in billions.
Over this past year, we have all come to wonder what we can do to make a difference in the face of problems that seem so overwhelming. When we think about the scope of the pandemic and other global health issues, the devastating numbers are heart breaking, and it’s easy to lose sight of the individual people and stories behind the statistics. In Aaron Berkowitz’s new book, “One by One by One,” he shares with us the lessons he learned as he tried to make a small difference by helping one individual at a time amid suffering measured in billions.






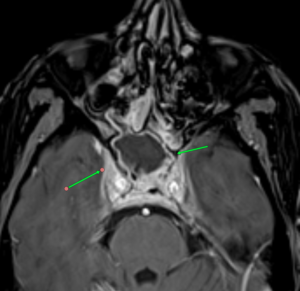
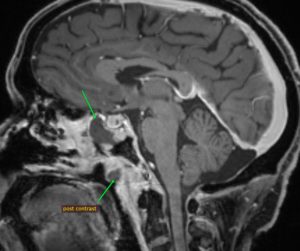
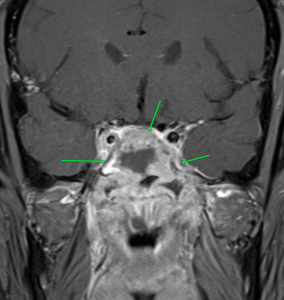 MRI images of mucormycosis with cavernous sinus involvement in a patient with COVID-19.
MRI images of mucormycosis with cavernous sinus involvement in a patient with COVID-19.

 The COVID pandemic had universal effects on medicine, and Mumbai was no exception. In fact, being a densely populated city with lots of international travelers, the cases appeared early and the magnitude was high, throwing the health system off gear.
The COVID pandemic had universal effects on medicine, and Mumbai was no exception. In fact, being a densely populated city with lots of international travelers, the cases appeared early and the magnitude was high, throwing the health system off gear.
