
Wolfgang Grisold
By Wolfgang Grisold and Steven Lewis
A worldwide concept for regional training
The mission of the World Federation of Neurology (WFN) is to foster quality neurology and brain health worldwide by promoting global neurological education and training. The WFN Education Committee has developed a concept paper to define the standards and requirements for WFN Training Centers worldwide. The purpose is to establish worldwide standards of neurological care and at the same time improve local training in neurology.
WFN Training Centers will provide excellent training in neurology regionally in all parts of the world. To be accredited by the WFN, centers must be public, openly accessible university centers. Neurology must be a department on its own, closely connected to related fields, such as neurosurgery, internal medicine, psychiatry, radiology and neuropathology.
Departments should have a defined structure of experience in general neurology, dealing with the most common neurological diseases worldwide, and also addressing local neurological needs. Training must be performed in inpatient and outpatient services. In addition, electrophysiology, neuro-ultrasound and CSF analysis should be available in the department. The objective of the training course should be the independent, unsupervised practice of neurology by the trainees after the termination of their training.
The center needs to provide the WFN with a detailed plan of the training, the teaching staff and the availability of departmental facilities and structural facilities for the WFN trainees, including a detailed description of housing and accommodations, legal issues, working permit and insurance.
Prior to the establishment of a WFN Training Center, the center must follow the accreditation process set by the WFN. This includes the submission of a formal application and detailed report about the center, written and face-to-face interviews with center staff and a site visit by representatives of the WFN.
The WFN, as a charity registered in the U.K., will only grant accredited status to a center after a thorough examination. The WFN expects that the Training Centers will conduct their programs in a responsible and economic way, in line with the WFN’s charitable aims.
Training Centers make regular reports to the WFN about the development of the trainees and confirm the end of training or other agreed milestones. WFN Training Center accreditation is for a period of two years and can be renewed.
Positions for future trainees at WFN Training Centers will be announced on the WFN website and on social media. The selection of candidates will be made by a committee composed of local/regional representatives and members of the WFN Education Committee.
Visit the WFN website for more information about WFN Training Centers.


















 by Antoaneta J. Balabanov
by Antoaneta J. Balabanov
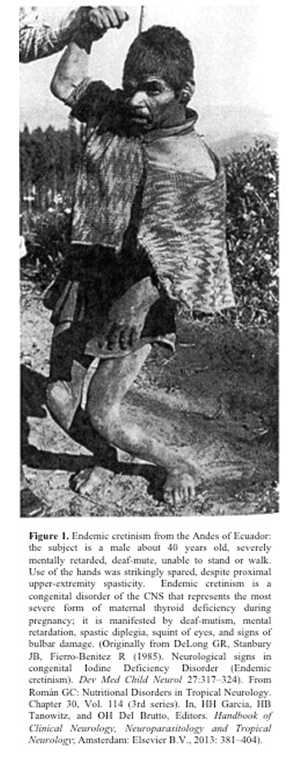 Encouraging news for the prevention of autism emerged from the results of a research study conducted by an international collaborative team conformed by Prof. Gustavo C. Román, MD, from the Methodist Neurological Institute (Houston, Texas) and researchers from the Generation R Study at Erasmus University Medical Centre in Rotterdam, The Netherlands, including Akhgar Ghassabian, MD, PhD; Jacoba J. Bongers-Schokking, MD, PhD; Vincent W.V. Jaddoe, MD, PhD; Albert Hofman, MD, PhD; Yolanda B. de Rijke, PhD; Frank C. Verhulst, MD, PhD; and Henning Tiemeier, MD, PhD. The results point to the deficiency of maternal thyroid function during the first trimester of pregnancy as a significant factor in the causation of autism in the child. Pregnant women with deficient thyroid hormone are nearly four times likelier to produce autistic children than women with normal thyroid function. The study was published in the prestigious journal Annals of Neurology1.
Encouraging news for the prevention of autism emerged from the results of a research study conducted by an international collaborative team conformed by Prof. Gustavo C. Román, MD, from the Methodist Neurological Institute (Houston, Texas) and researchers from the Generation R Study at Erasmus University Medical Centre in Rotterdam, The Netherlands, including Akhgar Ghassabian, MD, PhD; Jacoba J. Bongers-Schokking, MD, PhD; Vincent W.V. Jaddoe, MD, PhD; Albert Hofman, MD, PhD; Yolanda B. de Rijke, PhD; Frank C. Verhulst, MD, PhD; and Henning Tiemeier, MD, PhD. The results point to the deficiency of maternal thyroid function during the first trimester of pregnancy as a significant factor in the causation of autism in the child. Pregnant women with deficient thyroid hormone are nearly four times likelier to produce autistic children than women with normal thyroid function. The study was published in the prestigious journal Annals of Neurology1.