By Wolfgang Grisold
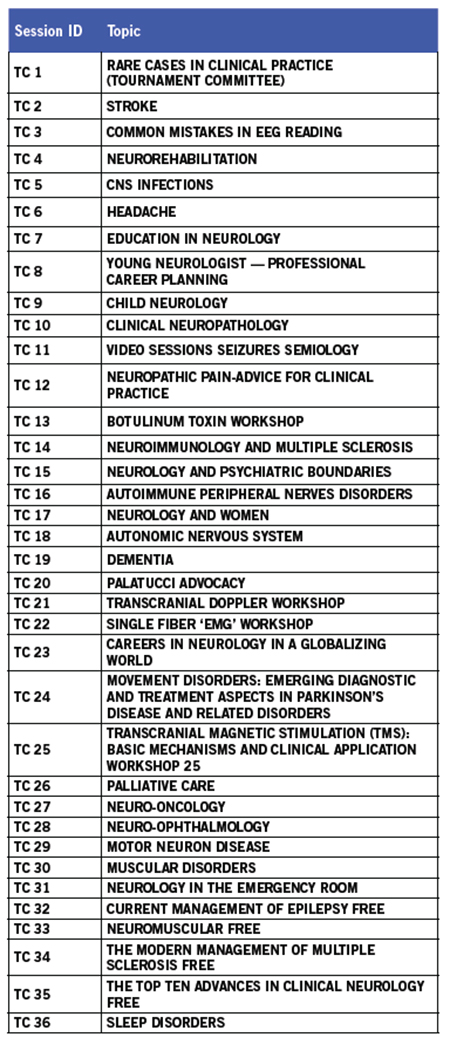
Table 1: Teaching Courses The free early morning teaching courses have remained the most visited teaching courses, despite the early hour. Teaching courses on education, advocacy and career received little attendance, yet these topics are inherent topics of the WFN. Also, palliative care received little attention as teaching courses. This shows that the topic needs promotion within the scientific sessions. All teaching courses will be available on the WFN website after the Congress.
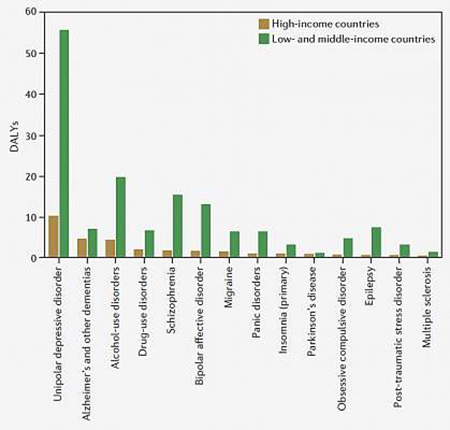
The WCN took place Oct. 31-Nov 5, 2015, at the CasaPiedra Conference Center in Santiago, Chile, with 3,500 delegates from 112 countries participating and creating a joint sense of neurology worldwide. The lectures from the World Health Organization (WHO) and the presentation of the new WHO Atlas of Neurology showed the disparity of neurological workforces around the world and documented the importance of the WFN activities in the work with global organizations. One of the goals and aims of the WFN is to spread neurological development and neurological science and update participants on current issues, but also to highlight new neurological fields of development.
Scientific sessions and topics are an excellent venue and bring participants close to the leading persons in the field. This concept was successfully used in plenary lectures and scientific main topic sessions.
The WFN also has long kept the tradition of offering teaching courses at its congress. This concept has been broadened since Marrakesh, as the WFN teaching courses now are being offered on all days of the congress. The teaching courses were co-chaired by Sergio Castillio (local committee, Chile) and Wolfgang Grisold (teaching course committee, WFN). The topics presented include many general and common topics, such as stroke, dementia, epilepsy and others.
Also, several courses with hands-on opportunities were offered to include and engage participants in practical issues, such as EMG, ultrasound and botulinum toxin treatment. Experience at the WCN in Marrakesh and Vienna has shown that these types of highly interactive teaching courses, despite often technical issues and difficulties, are well appreciated by attendees.
In Chile, 36 teaching courses were held. The list (Table 1) shows the topics presented, which helped to disseminate educational news and expert knowledge. Teaching courses offer attendees the advantage of being in a smaller group and interacting with renowned experts. This facilitates a climate of interaction by allowing questions and discussion of opinions.

Dr. Freedman lectures on education.
One special component of the WCN teaching courses are the early morning free teaching courses, a one-hour teaching session presented by a single expert in the field. This expert has the privilege to create his or her talk in the form of a lecture, deviating from the usually shorter teaching course lectures, and allowing the speaker to emphasize and shape the message that he or she considers important. Despite the early time of these teaching courses, the number of participants was between 100 and 200 per course (and 339 for the topic of epilepsy). The topics included MS (95), chronic inflammatory demyelinating polyneuropathy (125) and the top 10 advances in neurology (95).
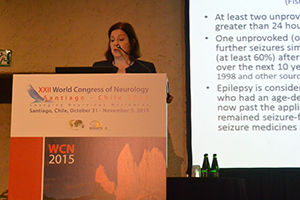
Cynthia L. Harden presents a morning teaching course on epilepsy.
Knowledge, skills and tutoring from experienced lecturers cover many aspects of neurology. The issue of palliative care is a topic with an increasing scientific basis1. Still palliative care is often confounded with end of life care, or worse, a situation of helplessness. The WFN has established a Research Group on this topic, and the Teaching Course on palliative care was an important step in establishing this important topic into our future curricula.

Dr. Nitrini speaks on education in Latin America.
All neurologists, working in any part of the world, also are aware of the importance of training, lecturing and teaching, and also that the diversity of careers from hospital to consultant level and from academic career to nonacademic career is wide. For this reason, a teaching course on education in neurology covered the topics on how to establish a curriculum, as well as how to integrate neurologic knowledge and procedures into the national situation, politics and legislation. It is important to define new learning strategies and teaching methods, to eventually support or replace the traditional apprenticeship model of neurologic education. Also the classic concept of knowledge, skills and competence will need to include aspects of professionalism and attitude. Knowledge is acquired in an incremental, almost pyramidal way. Yet, individuals and institutions also will need to adapt to new developments, and this procedure of systemic approach to replace old content or procedures is termed unlearning

Several speakers and participants gather for a photo opp.
One lecture by Dr. Freedman focused on the merging and growing possibilities of e-learning. He presented his own experience with video conferences worldwide and gave important clues to enlarge the scope of this project.
The local flavor of Latin American neurology was presented by Prof. Nitrini of Brazil, who outlined educational activities in Latin America. He discussed the rise of impact factors among publications from Latin America in the past years.
Within the topic of applied teaching and education, translation was discussed by Prof. Camfield of Canada. This term describes the often difficult transfer of young patients from pediatric neurology into adult neurology. Translation also has been well described in other fields of pediatrics and demonstrates a clash of concepts between different concepts of patient care and involvement of careers.

Prof. Raad Shakir outlines the role of the WFN in the Palatucci course.
Patient advocacy is an emerging concept, which empowers physicians to not only be involved in the provision of the best medical care, but also to advocate for patients in the micro- and macro-environment. This concept in neurology is carried forward by the American Academy of Neurology (AAN) Palatucci courses in the United States, and the AAN and WFN implemented a joint AAN-WFN one-day course in Chile. Topics on advocacy, press work and presentations were given to a small, but soon to be powerful group. Also WFN President Raad Shakir presented his concept of worldwide engagement of the WFN in health matters.

A good turnout attends a day of programming.
Last but not least, some of the most important targets of education are patients and caregivers. Despite the importance of these groups, patient awareness days are, surprisingly, often not included in congresses. Since WCN 2015, the WFN implemented a patient day into it congresses. This year’s topics included stroke, epilepsy, MS and dementia, and WFN Past-President Vladimir Hachinski served as convenor and engaged in the discussion.
Footnote
- Oliver DJ, Borasio GD, Caraceni A, de Visser M, Grisold W, Lorenzl S, Veronese S, Voltz R. “A consensus review on the development of palliative care for patients with chronic and progressive neurological disease.” Eur J Neurol. (Oct 1, 2015): doi: 10.1111/ene.12889).







 “Nothing we can do.” This is a commonly used phrase when discussing the management of amyotrophic lateral sclerosis with recently diagnosed patients. It is often uttered at a time when patients are at their most vulnerable. They have just discovered they have a relentlessly progressive neurodegenerative disease and simultaneously they are left with the impression that they are on their own because there is “nothing we can do.”
“Nothing we can do.” This is a commonly used phrase when discussing the management of amyotrophic lateral sclerosis with recently diagnosed patients. It is often uttered at a time when patients are at their most vulnerable. They have just discovered they have a relentlessly progressive neurodegenerative disease and simultaneously they are left with the impression that they are on their own because there is “nothing we can do.”


 The big drive of WHO toward global coordinating GCM NCDs is gathering pace. Although the scope of the process is not yet complete, one can see WHO trying to listen to all stakeholders, and the matter of WHO dealing with disease management is now a reality. The United Nations has produced the declaration on NCDs and 17 Sustainable Development Goals (SDGs) in 2015. In all these initiatives and targets, brain health should be at the forefront, and we as neurologists should push hard to have neurological issues right in the middle of governmental thinking. Financial support for our patients will only come if we have clear publically supported initiatives in a language that makes sense and shows targets, which are realistic and achievable.
The big drive of WHO toward global coordinating GCM NCDs is gathering pace. Although the scope of the process is not yet complete, one can see WHO trying to listen to all stakeholders, and the matter of WHO dealing with disease management is now a reality. The United Nations has produced the declaration on NCDs and 17 Sustainable Development Goals (SDGs) in 2015. In all these initiatives and targets, brain health should be at the forefront, and we as neurologists should push hard to have neurological issues right in the middle of governmental thinking. Financial support for our patients will only come if we have clear publically supported initiatives in a language that makes sense and shows targets, which are realistic and achievable.