Prof. Wolfgang Grisold highlights upcoming elections, global activities, World Brain Day, and educational efforts.
I hope you have had a nice summer, and all your work has been rewarding. For the World Ferderation of Neurology (WFN), the past months have been successful, and I want to update you on the upcoming Council of Delegates (COD) meeting, global activities, World Brain Day (WBD) 2024, education, and future meetings.
COD Meeting
This year’s COD meeting will convene on Sept. 25, 2024. A new trustee will be elected, replacing Prof. Alla Guekht, who successfully completed two terms as a trustee. Prof. Guekht has been very active, and during her term she has contributed enormously toward advancing the WFN in the global arena, working with the World Health Organization (WHO) and the U.N. Economic and Social Council. Prof. Guekht’s mission for global neurology was successfully supported by WFN intern Dr. Ksenia Pochigaeva, who monitored and updated us on important events.
The WFN board consists of four officers, three elected trustees, and up to two co-opted trustees. The trustees are regulated by the U.K. charity law, and they bear full personal responsibility for their tasks. The elected trustees may opt to elect two co-opted trustees for one year. These elections depend on requirements such as balance of the regions, gender, or other specific issues. This year’s co-opted trustees are Prof. Maria Benabdeljlil (Morocco) and Prof. Minerva Ruiz (Mexico).
The vote for the elected trustee position will be electronic, with six candidates applying for the position. (Read their statements.) These candidates have been scrutinized and recommended by the WFN Nomination Committee.
WFN leadership will undergo major changes in 2025, with terms ending for the president, past president, and one trustee. With a change of this magnitude, we need to ensure continuation on both the ends of the president’s term will be implemented. To facilitate this continuation, we suggest having the president-elect voted on one year earlier, and having the past president continue for another year, with both serving as advisors on the board. This suggestion will be made as a motion at the COD meeting by the trustees this year.
The WFN as a global organization has many long-term projects and responsibilities for global activities as well as education and meetings. For a simple overview, we have created a page to help guide visitors through the WFN activities.
In addition to the trustees’ reports, several committees will present their reports at the COD meeting. The financial audit (a yearly report for the U.K. Charity Commission) will be sent in advance, and delegates will be able to ask questions and give their final approval.
At this time, there will also be a call for the World Congress of Neurology (WCN) 2029, which will take place in Europe.
Global Activities

(Left to right) Prof. M. Benabdeljlil, Prof. Riadh Gouider, Natacha Kiswendsida (epilepsy trainee), Prof. Wolfgang Grisold, and Dr. Steven Lewis.
Global activities continue jointly with the WHO and the U.N. ECOSOC. On July 8, 2024, the WHO IGAP Toolkit was released. The WFN was honored to be a speaker at the release, which was a successful presentation of longstanding developments and will help all stakeholders implement the IGAP project. There are many entry points to the project, and all WHO member states will have the opportunity to adapt the IGAP to their needs by using this toolkit.
The main pillars of the IGAP are advocacy, prevention, therapy, research and development, and public health. These pillars provide opportunities for all to participate and reach the goals. As with our participation in the development and support of the toolkit, the WFN has taken the IGAP as a personalized agenda to move and develop further, and we welcome the WHO’s strong engagement in neurology. This is a unique opportunity, and the IGAP will continue to be a permanent platform for global neurology that will aid in implementing neurology and neurology services in all countries in need.

(Left to right) Prof. M. Benabdeljlil, Prof. Riadh Gouider, Dr. Mundih Njohjam (epilepsy trainee), Prof. Wolfgang Grisold, and Dr. Steven Lewis.
At the U.N. ECOSOC meeting in New York, the WFN was represented by Prof. Guekht. This United Nations High-Level Political Forum (HLFP) on sustainable development took place July 8-17, 2024, under the auspices of the ECOSOC. The main theme of the ECOSOC was “Reinforcing the 2030 agenda and eradicating poverty in times of multiple crises: the effective delivery of sustainable, resilient, and innovative solutions.” The WFN submitted a written statement on “Advancing Brain Health for Sustainable Development: A Call to Action.”
WBD Activities
WBD 2024 featured the topic “Brain Health and Prevention,” and followed our series of WBDs promoting brain health. It added to previous important features such as disability, which was the theme in 2023. Both dedicated WBDs have left us with many suggestions and tasks. We have learned that disability is more common than we assume. The recent update of the Global Burden of Disease has confirmed this and increased the spectrum from 17 to 34 neurological conditions.1 Disability in neurological disease not only includes long-term care and rehabilitation, but also the prevention of neurological diseases and avoidance of stigma.
Prevention, which was chosen for this year’s WBD, is a powerful tool that may be underused. We have seen many examples, including stroke, cerebrovascular disease, and several others. Recently, we have been exposed to many prophylactic recommendations to prevent dementia.2 In addition, we also face the introduction of new therapies, and we hope to gain strength and competence in these important areas to prevent and even cure dementia.
As with any biological condition, there are factors that can be modified, and others that can not. The impact of aging on cell biology and on the body are well known to neurologists. Many age-related factors, such as brain volume, cognitive capacities, performance of the neuromuscular system, and posture and gait, are implicitly incorporated into our daily work. We are aware that brain function in aged individuals varies, depending on many factors. The topic of aging and senescence is important for all parts of the body.3 Insight into these mechanisms will be important for future research.
As the age pyramid affects all global regions, this is a common issue for neurology worldwide. In addition to research, prevention, and care, we must also be aware to prevent ageism as brain health concerns the entire life span.4
Please see our report on WBD 2024. The webinar was attended by 1,000 participants. See a list of selected articles about WBD. (See Table 1 at the bottom of the page.)

Several awards for brain health projects were presented during a meeting of the Chinese Society of Neurology.
Chinese Society of Neurology
The Chinese Society of Neurology set aside July 21, 2024, to celebrate brain health and prevention. The event featured a large meeting with keynote lectures and several dedicated sessions about brain health at the China National Convention Center in Beijing. The theme was “World Brain Day 2024: Brain Health and Prevention.” The goals were to enhance public awareness of brain health, foster scientific advancement in brain health, and prevent and treat significant neurological and psychiatric disorders, including cerebrovascular diseases, cognitive disorders, and depression. There was also a focus on children’s brain development.
The conference invited prominent experts and scholars from both domestic and international arenas. Their presentations brought focus to the latest research advancements. There were also themed forums that presented and explored 12 specialized reports from various angles.

On WBD, Beijing Tiantan Hospital offered a free neurologic consultation day.
During the meeting, several awards for brain health projects were presented. On WBD, Beijing Tiantan Hospital offered a free neurologic consultation day that was well attended. Please also see the JNS WFN service page for more details.
WFN Educational Activities
We invite you to participate in the WFN’s educational activities. The e-Learning Hub has now received an improved, user-friendly interface, which will help guide all users of our website to engage in our archive and see past educational activities. Users can also connect to ongoing international activities.
The WFN Digital Neurology Update (WNU) takes place virtually Sept. 26-27, and serves as an update platform for neurology. There will be six plenaries from world-renowned experts on stroke, epilepsy, movement disorders, multiple sclerosis, headache, and dementia. During a break, attendees will have the opportunity to see industry and society events. Each day will conclude with six teaching courses in the afternoon. These will focus on important topics such as stroke, epilepsy, neuromuscular disorders, headache, the autonomic system, and the emerging topic of neuroepidemiology. All registered participants will be able to see all six teaching courses.

AFAN group photo after the closing ceremony.
For October, we plan a joint session with the World Stroke Organization (WSO) at the World Stroke Congress in Abu Dhabi. The session will focus on palliative care in stroke, which confirms the WFN’s major interest in disability, long-term care, and palliative care.
The International Congress on Neuromuscular Diseases (ICNMD), the WFN’s neuromuscular congress, will be held Oct. 25 in Perth, Australia. After circulating the globe, the ICNMD has found excellent hosts in Perth and will present a congress incorporating all parts of the neuromuscular system, such as motor neuron disease, peripheral nerves, neuromuscular transmission, and muscle. We expect an exciting program. For those unable to travel to this destination, we will provide a virtual program that will cover the highlights.
Jointly with the International Headache Society, Global Patient Advocacy Coalition, the American Migraine Foundation, and the African Academy of Neurology (AFAN), we will continue our e-learning days on headache. The next session, Education in Headache to Health Care Professionals in Africa, is planned for Nov. 23, 2024. Register for the free session.
Early in 2025, we will have a joint educational day with the Asian and Oceanian Association of Neurology (AOAN) on movement disorders, autoimmune diseases, and the brain.

Prof. Gallo Diop receives the acknowledgement from WFN President Prof. Wolfgang Grisold.
We supported and attended the July meeting of AFAN in Dakar. There was a joint education session with AFAN on Africa, and Prof. Gallo Diop was honored by the WFN.
We also conducted a site visit at our successful WFN Training Center in Dakar. Interviews with the staff and the trainees confirmed the high level of the training center. Please read more on the educational situation in the WFN service pages in the Journal of the Neurological Sciences.
The WFN continuously offers positions for training in our WFN Training Centers. For Cape Town, a new four-year training position was announced in July 2024. The position generated 165 applications, which is a new record of interest.
Jointly with the AAN, the WFN is developing a global program for Advocacy and Leadership for low middle and low income countries. You can find more information on the WFN website.
Please follow our website, social media, and the JNS WFN service page for more news from WFN. •
Table 1. Organizations and publications featuring WBD articles.
|
Organization or Publication |
Article Title |
Link |
|---|---|---|
|
The Lancet |
World Brain Day 2024: A Focus on Brain Health and Prevention |
https://www.thelancet.com/journals/laneur/article/PIIS1474-4422(24)00270-9/fulltext |
|
WFN |
World Brain Day 2024 |
|
|
PR Newswire |
2024 World Brain Day Dedicated to Brain Health and Prevention |
|
|
Journal of Neurological Sciences |
World Brain Day 2024: Promoting Brain Health and Prevention |
https://www.jns-journal.com/article/S0022-510X(24)00230-2/abstract |
|
EPNS |
World Brain Day 2024 |
|
|
National Library of Medicine |
Wolrd Brain Day 2024: A Focus on Brain Health and Prevention |
|
|
WFN |
World Brain Day: Background |
|
|
National Today |
World Brain Day 2024 |
|
|
World Neurology |
World Brain Day 2024: Promoting Brain Health and Prevention Globally |
|
|
Revival Research Institute |
World Brain Day 2024: Tips to Improve Your Brain Health |
|
|
UBC News |
World Brain Day 2024: Protecting Our Future |
https://events.ubc.ca/event/world-brain-day-2024-protecting-our-future/ |
|
Science Open |
World Brain Day 2024 |
|
|
Aspire |
World Brain Day 2024 |
|
|
Medindia |
World Brain Day 2024: Advocating for Brain Health and Prevention |
|
|
American Brain Foundation |
World Brain Day: 4 Simple Ways to Support Brain Health |
https://www.americanbrainfoundation.org/world-brain-day-4-ways-to-support-brain-health/ |
References
1. Collaborators, GBD. Nervous System Disorders. 2024. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol.
2. Livingston G, Huntley J, Liu KY, Costafreda SG, Selbaek G, Alladi S, Ames D, Banerjee S, Burns A, Brayne C, Fox NC, Ferri CP, Gitlin LN, Howard R, Kales HC, Kivimaki M, Larson EB, Nakasujja N, Rockwood K, Samus Q, Shirai K, Singh- Manoux A, Schneider LS, Walsh S, Yao S, Sommerlad S, and Mukadam N. 2024. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet.
3. Ogrodnik M, Carlos Acosta J, Adams PD, d’Adda di Fagagna F, Baker DJ, Bishop CL, Chandra T, Collado M, Gil J, Gorgoulis V, Gruber F, Hara E, Jansen-Durr P, Jurk D, Khosla S, Kirkland JL, Krizhanovsky V, Minamino T, Niedernhofer LJ, Passos JF, Ring NAR, Redl H, Robbins PD, Rodier F, Scharffetter-Kochanek K, Sedivy JM, Sikora E, Witwer K, von Zglinicki T, Yun MH, Grillari J, and Demaria M. 2024. Guidelines for minimal information on cellular senescence experimentation in vivo. Cell 187 (16):4150- 4175.
4. Marques, S, Mariano J, Mendonca J, De Tavernier W, Hess M, Naegele L, Peixeiro F, and Martins D. 2020. Determinants of Ageism against Older Adults: A Systematic Review. Int J Environ Res Public Health 17 (7).









 The
The 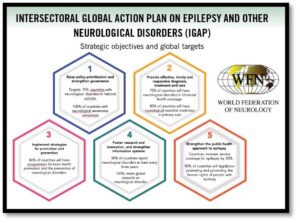 The EPNS strives to foster, expand, and support science and clinical research in child neurology by bringing together the best clinicians and scientists in the field. This includes the society’s flagship
The EPNS strives to foster, expand, and support science and clinical research in child neurology by bringing together the best clinicians and scientists in the field. This includes the society’s flagship  Medications and services can be costly and difficult to obtain for many Honduran patients.
Medications and services can be costly and difficult to obtain for many Honduran patients. On the occasion of World Brain Day (WBD) 2024, a brain health conference was held July 20-21, 2024, at the China National Convention Center in Beijing. The conference was centered on the theme of “World Brain Day 2024: Brain Health and Prevention.” The goal was to enhance public awareness of brain health, foster scientific advancement in brain health, and prevent and treat significant neurological and psychiatric disorders.
On the occasion of World Brain Day (WBD) 2024, a brain health conference was held July 20-21, 2024, at the China National Convention Center in Beijing. The conference was centered on the theme of “World Brain Day 2024: Brain Health and Prevention.” The goal was to enhance public awareness of brain health, foster scientific advancement in brain health, and prevent and treat significant neurological and psychiatric disorders.