Donald H. Silberberg
As we begin to think about attending the forthcoming World Congress of Neurology in Santiago, Chile, it seems timely to consider how we might take advantage of the unique opportunity that this provides to advance our field. As WFN President Raad Shakir points out in his column in this issue of World Neurology, we neurologists everywhere attempt to address identical or very similar clinical problems, but in quite different environments. Some do so surrounded by colleagues and all of the support systems that are key to optimal care. Others of us walk alone, sometimes as the sole neurologist in a region with very few physicians. Because of differences in the local health care system, cultural and other environmental differences, the neurologist practicing in optimal circumstances thinks about epilepsy, Parkinson’s disease or stroke in quite a different way than her counterpart practicing in difficult circumstances or in conflict zone.
A major function of an international meeting such as the World Congress of Neurology is to facilitate the sharing of knowledge, and to help develop ongoing working relationships that can lead to many advances for all. Although publications and electronic communications provide essential ways to communicate, an international meeting offers unparalleled access to one’s peers whose workplace and problems are far from home, but may be extremely informative.
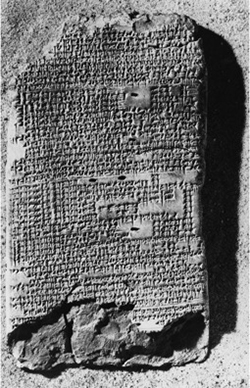
Both information sharing and clinical and research collaboration become very real possibilities. Clinical collaboration today often takes the form of setting up periodic video conferences, supplementing important opportunities to visit one another. Research collaboration can lead the way to developing multilateral programs supported by universities, national agencies such as the National Institutes of Health (U.S.) or Canada’s Grand Challenges Program, and foundations such as the Bill and Melinda Gates Foundation. Many of us engaged in global neurology can think back to ways in which WFN congresses and other meetings introduced us to international problems, opportunities and colleagues—let’s put WCN Santiago to work for this purpose in November.