By Peter J. Koehler

Christiaan Huygens; painting by Caspar Netscher (public domain).
Many famous persons, today as well as in the past, suffer(ed) from migraine. With a prevalence of around 16% for women and 8% for men, it ranks high in the Global Burden of Disability.1 Going back in history, it may be difficult to make a retrospective diagnosis, in particular, if not all symptoms, as described in current diagnostic classifications, are mentioned. However, the disability can often be recognized quite easily, as in the following case. In this essay, I will discuss a 17th century scientist, who was suffering from frequent headaches, possibly migraine.
Conversation in Latin at Age 9
Christiaan Huygens (1629-1695) was born in The Hague (Netherlands) as the second son of Suzanna van Baerle (1599-1637) and Constantijn Huygens (1596-1687), who had been a diplomat and secretary of two Princes of Orange. Constantijn was also a poet and composer. He was interested in the arts and is considered by some the discoverer of the talent of Rembrandt (and Lievens), who at the time were working in nearby Leyden. He was acquainted with Descartes and played an important role in the publication of his Discours de la méthode (Dioptics). Most probably, they first met at Hofwijck castle, Huygens’ summer residency just outside of The Hague, in May 1642. Descartes wrote about Constantijn Huygens. “The honour to know him I cherish as one of the most happy things that happened to me.” Huygens wrote about Descartes: “Truly, he is a man superior to all esteem that one would wish to render him.”
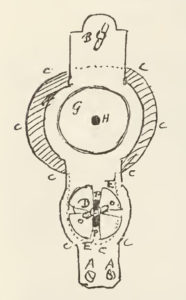
Design for a microscope in letter to his brother Constantijn 1678.9
Christiaan was educated at home and excelled in nearly all subjects. He was able, for instance, to converse in Latin at age 9. Following a two-year study period of law and mathematics at Leyden University, he continued his studies at the Orange College in Breda. Despite his father’s wish to become a diplomat, Christiaan was interested in mathematics rather than law. He, as well as his father, corresponded with the French philosopher and mathematician Marin Mersenne (1588-1648). Constantijn called his son “mon Archimède,” in imitation of the Mersenne, who had noticed the remarkable gift of young Christiaan and encouraged him to continue his mathematical studies.
Designs for an Improved Microscope

Brass microscope with five diaphragms and object revolver for six specimens after design by Christiaan Huygens (c 1680). Courtesy Boerhaave Museum, Leiden (V 26952).
Thus, Christiaan became famous as mathematician, physicist (considered a founder of mathematic physics), and astronomer, who corresponded with and became Fellow (1663) of the Royal Society (London), as well as member (and research director) de l’Académie des Sciences (Paris). At the latter academy, he was served and paid by King Louis XIV. Christiaan invented the pendulum clock2 and described light as a wave phenomenon;3 moreover, he discovered the moon Titan of Saturnus (1655; publication of De Saturni Luna observatio nova in 1656). He constructed a variety of optical instruments, often in close association with his older brother Constantijn.4 He not only used telescopes, but was also interested in microscopes. Already in the 1650s, the brothers had compound microscopes. Christiaan’s enthusiasm for this instrument increased after he had translated and presented the work of Antoni van Leeuwenhoek at the Paris Académie. He also wrote to Nehemia Grew (1641-1712), the Secretary of the Royal Society in London, that he “directed [his] mind to constructing a new microscope, excited by that new observation, which shows that the semen is full of living vivacious animalcula.”5 As Van Leeuwenhoek’s letter was published in the Philosophical Transactions only a year after receipt, Huygens’ short description became the first.4 Not satisfied with Leeuwenhoek’s original instrument, Huygens made six designs of an improved simple microscope with a diaphragm revolver as well as a specimen revolver. The improvement concerned the quality of the image and the manipulation of the specimens.4 In August 1678, he wrote to his brother about a more practical type of microscope. The design was used by several instrument makers.
Incapacitating Headache
In the 22-volume Oeuvres Complètes (OC 1888-1950), that includes his correspondence (in Latin, German, English, and Italian) and writings, mainly written in (old) French, interesting information can be found about his chronic headache.
In 1652, in a letter to Frans van Schooten junior, who was professor of mathematics at the University of Leyden, Christiaan wrote about his headaches for the first time. He must have been 23 years old. Due to headache that was not always present, but occurred at the most inconvenient moments, he was often unable to work, unless he was able to overcome the pain by willpower. About 10 years later, we learn about the treatment that was applied as advised by his physician. In a letter to his younger brother Lodewijk, he complained about his headaches and mentioned that he had had himself bled and purged. These kinds of treatments were indeed quite common and should be explained in the context of contemporary humoral medicine.7
Since my latest [letter] I have taken advise of our medic Libergen [sic], who had me purged and bled, having done that, I had a nasty cold as I have never known to have had, in such a way that I not only have to stay at home, but also have to abstain from reading, writing, or meditating, because as soon as I do I have a headache.
The Liebergen family counted numerous physicians. Huygens probably referred to Willem van Liebergen (1601-1674), who had studied philosophy and medicine at Leyden University.
Christiaan had to apologize himself regularly for his behavior due to headache. After he moved to Paris and became a member of the new Académie Royale des Sciences, he wrote to the husband of his sister Susanna that due to headache, he had been unable to write him, although he usually was punctual with this respect. He still felt some remnants of the latest period.
A few months later, in November 1666, he wrote to the same person that writing caused headache. In 1677, Constantijn sr. wrote about his son’s health. “My Archimedes has recovered well enough from his ailment, although always frail and subject to headaches.” A year later, Constantijn jr. wrote, “My brother has a severe headache.” At age 56, Christiaan was still suffering from headaches, writing “I have written a part of the memoirs, as you know and would have completed it without headaches that, since Easter day, have annoyed me and by which, still today, I did not go outside.”
Half a year later, he wrote again to his brother Constantijn that “since three days there is a constant fog here that gives me very annoying migraines.” In the spring of 1686, he wrote to the same brother that next to an inguinal hernia, he was still suffering from headaches. “Meanwhile I am suffering as you may believe, in addition I have been tormented anyhow all these days by my migraines, that now begin to leave me.”
Correspondence With European Scientists
In his correspondence with many famous persons of the period, Christiaan sometimes referred to his headache. In January 1664, the French poet and critic Jean Chapelain (1595-1674), who also corresponded with Constantijn sr., wrote to Christiaan: “I am glad at least about the relief that you experienced with respect to you headache.” Toward the end of that year, Christiaan wrote to natural philosopher Sir Robert Moray (1608-1673), one of the founding members of the Royal Society, “Not having been able to respond in the usual way, I should not let leave the mail another time without acquitting myself of this duty despite an annoying headache that lasted this whole day and brings me in a mood of rather doing nothing.” Moray responded:
All your letters oblige me very much. However, your latest of the 21st does so even more than all previous ones. Writing me a long letter, full of nice things, while a headache tempts you not to do anything, well deserves to be estimated as a very special sign of extraordinary affection, it is therefore quite reasonable that I write a prompt and, as much as I can, satisfactory response.
And in 1692, in a letter to the German philosopher and mathematician Gottfried W. Leibniz (1646-1716), with whom he wrote on the mathematization of physics and on whom he had an important influence, he wrote: “I am very obliged for showing interest in my health, that since my last [letter] has suffered much from migraine during that long freeze.”
Mother and Sister Suffering Too
A hereditary factor may have played a role in Christiaan’s headache as his sister Susanna (1637-1725) wrote about her own migraine in 1680. “It is to my great regret, my dear brother, that I learn … that you have been uncomfortable by pain and heat in the head … I hope to learn soon that you will not complain anymore. I certainly have my part of migraine sometimes, and I complain more than anybody of those, who suffer of similar discomforts.” Christiaan and his sister may have inherited the affliction from their mother. She suffered from migraine and menstruation troubles, for which she had to be put a diet and was prescribed bleeding as well as purging.
Treatment With Water and Tea
In August 1654, Christiaan stayed in a spa in the mountains of the eastern part of the present Belgium. This was a well-known town with healing cold mineral springs since the 14th century that had resulted in the eponym spa. His father was staying there too and took water a couple of times. In one of the poems written for Mdm Emilia de Mérode-van Wassenaar during a stay, Constantijn Sr. wrote about migraine (1654):
Trouvez vous pas quelque migraine
Qui vous eschauffe le cerveau?
Si ma conjecture n’est vaine
Il vous reste tant soit peu d’eau
[Don’t you feel any migraine
That sets on fire your head?
If my diagnosis is right
Water is the only cure to save you]
Constantijn Sr. probably used the water more often than his son Christiaan, who was rather critical about its healing effects.
In the first half of the 17th century, tea was used as a remedy and reserved to high society. In the course of the century, however, it became more widespread and not just as a drug. Next to purging and bleeding, Christiaan indeed drank tea and apparently was satisfied about it. In 1663, still staying in Paris, he wrote to his brother Constantijn “If there is a way to send me … a pound or a half of the good tea, you would do me a great pleasure, as, since some weeks, I have felt myself admirably well by only taking the leafs in the mouth, as soon as I feel myself indisposed by headache, because that cures me without fail.” Furthermore, water cures, as usual at the time,7 were attempted.
Migraine and the Use of Optical Instruments
Letter by Huygens to Leibniz (1692) (from Oeuvres Complètes vol. 10, p. 268).
During the 19th century, migraine, in particular migraine with aura, was associated with scientists, who were using optical instruments. French physicist and astronomer Dominique François Jean Arago (1786-1853), Scottish physicist David Brewster (1781-1868), and British Astronomer Royal George Biddell Airy (1801-1892) are persons often referred to. Airy’s son, the physician Hubert Airy (1838-1903), who was also a victim to visual auras, believed it had its origin from their habits of accurate observation leading to intensive eye-work and brain-work, exposing them to the risk of impairment of the eyesight. He gave some striking descriptions of his own auras and added several figures of his experiences. The aura was emphasized rather than the headache. There is no indication that Huygens was suffering from auras.
Comorbid Depression
The recurrent episodes, some of which being clearly incapacitating, and familial occurrence suggest that Huygens was suffering from migraine, although some symptoms that would be expected were not described. Another aspect of his health was that he went through at least two periods of melancholia hypochondrica, notably in 1670 and 1676. Assuming we would diagnose this disease as a depressive disorder today, we know this is associated with migraine. And of course, melancholy was considered the disease of scholars at least in the century that started a few years after Christiaan Huygens’ decease in 1695. •
References
-
Steiner TJ, Stovner LJ, Jensen R, Uluduz D, Katsarava Z; Lifting The Burden: the Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD2019. J Headache Pain. 2020;21:137
-
Huygens C. Horologium Oscillatorium sive de motu pendulorum. Paris, Muguet, 1673.
-
Huygens C. Traité de la lumière, Leiden, Pieter v.d. Aa, 1690.
-
Fournier M. Huygens’ designs for a simple microscope. Annals of Science 1989;46: 575-596.
-
Huygens C. Oeuvres Complètes X. Correspondence of June 6, 1678. No. 2125 ; p. 77 (translation in ref. 3).
-
Koehler PJ. Huygens’ headache. Cephalalgia. 2015;35:1215-9.
-
Koehler PJ, Boes CJ. A history of non-drug treatment in headache, particularly migraine. Brain. 2010;133:2489-500.
-
Koehler PJ, Boes CJ. History of Migraine. In: Swanson et al. eds. Migraine. Handbook of Clinical Neurology. In press.
-
Huygens C. Oeuvres Complètes VIII. Correspondence of August 11, 1678. No. 2133 ; pp. 90-3.