By Abdul Malik, MBBS, DCN, MD

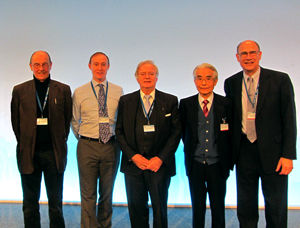
PSN conference organizers and faculty with Erik Wolters, Daniel Truong and R. Pfeiffer.
The specialty of neurology shows remarkable growth in last decade in Pakistan. The 21st meeting of the Pakistan Society of Neurology (PSN) was organized in collaboration with the International Association of Parkinson’s and Related Disorders (IAPRD) March 28-30 in Karachi, Pakistan.
There were eight scientific sessions and a half-day Botox Hands-On Workshop in this conference. The speakers from Netherlands, the United States, Saudi Arabia and Pakistan shared their experiences pertaining to neurology. The core of the discussion was the advances in movement disorders and the newer therapies now emerging. The guest faculty from the IAPRD had given a detailed overview on the topic.
An ample demonstration on patients was given with the title of “Botulinum Toxin Hands-On Use in Dystonia” by Prof. Daniel Truong from The Parkinson and Movement Disorder Institute (U.S.). He also delivered a lecture on Clinical Approach and Management of Dystonias. Prof. Ronald Pfeiffer, vice chair of the Department of Neurology at the University of Tennessee Health Science Center (U.S.) gave us an updated overview on Autonomic Dysfunction in Parkinson’s Disease and Drug-Induced Movement Disorders. The keynote speaker was Prof. Erik Wolters, IAPRD president, who is working in the Universities of Maastricht and Zurich. He delivered his lectures on the topics of Behavioral Dysfunction in Parkinson’s Disease and Parkinson’s Disease — Revisited.
More than 200 exceedingly participative audiences from all parts of the country attended all of the scientific sessions. In the inaugural session of the three-day conference, the Sardar Alam, outgoing Pakistan Society of Neurology (PSN) president, welcomed the delegates and presented the report of the last two years of the society’s works. Prof. M. Wasay, chairman of the organizing committee, stated the statistics of neurology care and neurologist in Pakistan. He said that for every one million people only one neurologist is available.
In the scientific sessions, Asif Moin, from Saudi Arabia, delivered the talk on utilization of SPECT and PET in epilepsy; Qasim Bashir discussed initial experience in establishing an interventional neurology/neuroendovascular surgery program in Lahore: procedural types and outcomes; Qurat Khan from AKU deliberated on introduction to behavioral neurology; Bushra Afroze talked on biotinidase deficiency — clinical presentation, diagnosis and treatment while neurodegeneration in children: diagnostic issues in developing countries was presented by Tipu Sultan from Children Hospital Lahore. A unique and thought-provoking session of this was in the Neurology Training and Advocacy session. This session highlighted the glimpses on post-graduate neurology in Pakistan by Sarwar Siddiqi, psychiatric care and interface with neurology by Prof. Iqbal Afridi, neurosurgery care and interface with neurology by Prof. Junaid Ashraf and advocacy for neurological care in Pakistan Prof. Rasheed Jooma.
There were 15 original oral presentations and 20 poster presentations from all major institutes of the country. This year, PSN officially had given best oral presentation and poster presentation awards. There was also an inaugural dinner in which the primary guest was Prof. Asghar Butt, vice president of CPSP. Prof. Masood Hameed Khan, vice chair of DUHS was honored during the social portion of the evening.
The conference was a great success in terms of participation, and the quality of training and education was superb.
 The 2014 Annual Meeting of the American Academy of Neurology (AAN) attracted more than 13,000 neurology professionals to Philadelphia, a city rich in its own neurology-related history. More than 2,500 presentations of cutting-edge research were available to attendees from across the world. The number of non-U.S. attendees was nearly 4,000.
The 2014 Annual Meeting of the American Academy of Neurology (AAN) attracted more than 13,000 neurology professionals to Philadelphia, a city rich in its own neurology-related history. More than 2,500 presentations of cutting-edge research were available to attendees from across the world. The number of non-U.S. attendees was nearly 4,000.
 It is a privilege to introduce the book “Electroencephalogram Examples and Guides,” published in August 2013. The book provides a concise and comprehensive compilation of text and EEG recordings collected to shorten the learning curve toward competence in EEG interpretation.
It is a privilege to introduce the book “Electroencephalogram Examples and Guides,” published in August 2013. The book provides a concise and comprehensive compilation of text and EEG recordings collected to shorten the learning curve toward competence in EEG interpretation.



 Elsevier already has introduced this feature, which is named “Your Paper Your Way (YPYW),” for several other journals in its portfolio. It has been so well received by authors that we will shortly begin offering this service to authors of manuscripts submitted to JNS. Taken together, these new options for manuscript formatting flexibility should make it easier for authors to submit manuscripts to JNS.
Elsevier already has introduced this feature, which is named “Your Paper Your Way (YPYW),” for several other journals in its portfolio. It has been so well received by authors that we will shortly begin offering this service to authors of manuscripts submitted to JNS. Taken together, these new options for manuscript formatting flexibility should make it easier for authors to submit manuscripts to JNS.



