HISTORY OF NEUROLOGY
By Edward H. Reynolds

Edward H. Reynolds
Samuel Alexander Kinnier Wilson (SAKW) (1878-1937) is distinguished throughout the neurological world for 1) the disease that bears his name, 2) his scholarly two-volume textbook which was published posthumously in 1940, and 3) his founding in 1920 of the Journal of Neurology and Psychopathology, now known as the Journal of Neurology, Neurosurgery and Psychiatry.
Born in New Jersey, to a Scottish mother and an Irish missionary Presbyterian Minister father, he returned to Scotland for his education. He graduated from the Edinburgh Medical School in 1902 and obtained a BSc with First Class Honors in Physiology in 1903. With a Carnegie Fellowship, he immediately proceeded to Paris for a year to study neurology under Pierre Marie at the Bicàªtre Hospital, followed by a few months in Leipzig. In 1904 he was appointed House Physician to the National Hospital for the Paralyzed and Epileptic in London and remained at the National Hospital for the rest of his career, as resident medical officer, registrar, pathologist, assistant physician, and finally full physician in 1921. In 1919, SAKW was also appointed junior neurologist to King’s College Hospital, one of the first of such posts in the UK to incorporate the word “neurologist.”
Samuel Alexander Kinnier Wilson (1878-1937).
In 1931, Sherrington invited SAKW to participate in a symposium on muscle tone at the first International Congress of Neurology in Berne. Sherrington and SAKW were elected as president and secretary-general respectively of the second International Congress of Neurology in London in 1935, but Sherrington later had to withdraw due to ill health. In 1933 Sherrington and his joint Nobel Prize (1932) winner, Adrian, both proposed SAKW for the fellowship of the Royal Society.
Pierre Marie (1853-1940). SAKW’s first influence in Paris.
Guided by his future father-in-law Alexander Bruce (1854-1911), an Edinburgh physician, with an interest in neurology, who also founded a neurological journal (Review of Neurology and Psychiatry 1903-1916), SAKW understood that Paris was the leading world neurological center at the turn of the 20th century. Hence, his seminal year (1904) influenced by Marie, Babinski, Dejerine and Meige among others, before proceeding to the National Hospital, Queen Square. He published his famous Edinburgh thesis on hepatolenticular degeneration (later called Wilson’s disease) in 1912, not only in Brain but also in Revue Neurologique. Furthermore he presented his work in French to the Société de Neurologie de Paris on Jan. 25, 1912, where it was very well received, but I cannot trace any record of a presentation to any UK society, such as the Section of Neurology of the Royal Society of Medicine in London. Just as Charcot had been a regular visitor to the UK in the late 19th century, so SAKW was a frequent visitor in the new century to France, where Crouzon, Guillain and Léri were particular friends and collaborators.
Octave Crouzon (1874-1938). SAKW’s contemporary and friend in Paris. (Courtesy of Emmanuel Broussolle).
It is interesting that even at the 17th International Medical Congress in London in 1913 the French delegation was the dominant influence in the Section of Neurology/Neuropathology, the proceedings of which were published in detail in Revue Neurologique but not in any English journal. Following that Congress SAKW and nine other British physicians were elected “Membres Correspondants Etrangers” of the Société de Neurologie de Paris, which had been founded in 1899.
In the last 25 years, I have had the privilege of working with SAKW’s son, James KW, a Cambridge-based assyriologist, on the subject of Babylonian neurology and psychiatry. Through James KW, I have learnt most about his father’s French connections. I have in my possession SAKW’s original seven-page brochure listing the members of the Société de Neurologie de Paris for 1926. It now includes 76 Paris-based neurologists, 60 French neurologists from beyond Paris and 128 international members from around the world, mainly Europe and the U.S./Canada, including 14 from the UK. Although the Neurological Society of London had been founded earlier in 1886 and had evolved in 1907 into the Section of Neurology of the Royal Society of Medicine, it had remained a small almost exclusively London-based Society. When the Association of British Neurologists (ABN) was founded in 1933, it had only 25 members.
References
Reynolds EH. Kinnier Wilson and Sherrington. J Neurol Neurosurg Psychiatry 2008;79:478-9.
Reynolds EH. Kinnier Wilson’s French connections. Rev Neurol 2014 Jun 3. pii: S0035-3787(14)00840-6. doi: 10.1016/j.neurol.2014.03.011.
Edward Reynolds is consultant neurologist and former director of the Institute of Epileptology, King’s College, London, and former president of the International League against Epilepsy. Peter J. Koehler is the editor of this history column. He is neurologist at Atrium Medical Centre, Heerlen, The Netherlands. Visit his website at http://www.neurohistory.nl










 by Antoaneta J. Balabanov
by Antoaneta J. Balabanov
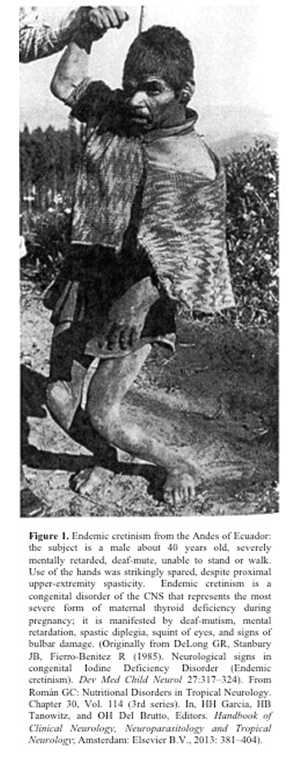 Encouraging news for the prevention of autism emerged from the results of a research study conducted by an international collaborative team conformed by Prof. Gustavo C. Román, MD, from the Methodist Neurological Institute (Houston, Texas) and researchers from the Generation R Study at Erasmus University Medical Centre in Rotterdam, The Netherlands, including Akhgar Ghassabian, MD, PhD; Jacoba J. Bongers-Schokking, MD, PhD; Vincent W.V. Jaddoe, MD, PhD; Albert Hofman, MD, PhD; Yolanda B. de Rijke, PhD; Frank C. Verhulst, MD, PhD; and Henning Tiemeier, MD, PhD. The results point to the deficiency of maternal thyroid function during the first trimester of pregnancy as a significant factor in the causation of autism in the child. Pregnant women with deficient thyroid hormone are nearly four times likelier to produce autistic children than women with normal thyroid function. The study was published in the prestigious journal Annals of Neurology1.
Encouraging news for the prevention of autism emerged from the results of a research study conducted by an international collaborative team conformed by Prof. Gustavo C. Román, MD, from the Methodist Neurological Institute (Houston, Texas) and researchers from the Generation R Study at Erasmus University Medical Centre in Rotterdam, The Netherlands, including Akhgar Ghassabian, MD, PhD; Jacoba J. Bongers-Schokking, MD, PhD; Vincent W.V. Jaddoe, MD, PhD; Albert Hofman, MD, PhD; Yolanda B. de Rijke, PhD; Frank C. Verhulst, MD, PhD; and Henning Tiemeier, MD, PhD. The results point to the deficiency of maternal thyroid function during the first trimester of pregnancy as a significant factor in the causation of autism in the child. Pregnant women with deficient thyroid hormone are nearly four times likelier to produce autistic children than women with normal thyroid function. The study was published in the prestigious journal Annals of Neurology1.

 This book reviews the history of the first 50 years of the WFN which was officially founded in 1957. One question immediately comes to mind: Why 1957? There may be a debate about the “date of birth” of neurology, but everybody agrees that it was firmly established as a discipline by the first part of the 20th century or even before that time. In subsequent years, there were several meetings attended by international members, even though the two World Wars forced the cancellation of some of these meetings. Why then did we have to wait until 1957 to see the foundation of WFN? One probable reason is that international collaboration, like international travel, was much less common than it later became. It took the strength and charisma of one man, Ludo van Bogaert, to carry through the creation of the federation. Note that in its early years, WFN was “worldly” only in name: Asia, Africa and Oceania were barely represented. Yet it was certainly quite international. A picture in the first pages of the book shows that of 10 delegates participating in an early WFN organizational meeting, one was from Cuba, one from Iran while a third was a neurosurgeon representing India. Iran and India were the only two Asian countries present in the initial years of WFN. In its first years, WFN survived mainly thanks to a grant from the US-based National Institutes of Health (NIH).
This book reviews the history of the first 50 years of the WFN which was officially founded in 1957. One question immediately comes to mind: Why 1957? There may be a debate about the “date of birth” of neurology, but everybody agrees that it was firmly established as a discipline by the first part of the 20th century or even before that time. In subsequent years, there were several meetings attended by international members, even though the two World Wars forced the cancellation of some of these meetings. Why then did we have to wait until 1957 to see the foundation of WFN? One probable reason is that international collaboration, like international travel, was much less common than it later became. It took the strength and charisma of one man, Ludo van Bogaert, to carry through the creation of the federation. Note that in its early years, WFN was “worldly” only in name: Asia, Africa and Oceania were barely represented. Yet it was certainly quite international. A picture in the first pages of the book shows that of 10 delegates participating in an early WFN organizational meeting, one was from Cuba, one from Iran while a third was a neurosurgeon representing India. Iran and India were the only two Asian countries present in the initial years of WFN. In its first years, WFN survived mainly thanks to a grant from the US-based National Institutes of Health (NIH).


